Project Purpose
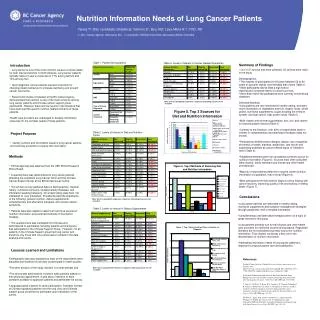
Nutritional Care of Lymphoma Patients Referred to BC Cancer Agency Oncology Nutrition in 2007: A Retrospective Analysis. Sekhon, I 1 , Sekhon, S 2 , Levy-Milne R 2. 1 University of British Columbia 2 BC Cancer Agency, Vancouver, British Columbia . Introduction. Summary of Findings.

Project Purpose
E N D
Presentation Transcript
Nutritional Care of Lymphoma Patients Referred to BC Cancer Agency Oncology Nutrition in 2007: A Retrospective Analysis Sekhon, I1, Sekhon, S2, Levy-Milne R2 1 University of British Columbia 2BC Cancer Agency, Vancouver, British Columbia Introduction Summary of Findings • From January 2007 to December 2007, there were 194 Lymphoma patients referred to BCCA Oncology Nutrition as identified under the CAIS code N/PLY. Thirty-eight patients were excluded from the study due to missing nutrition chart notes and/or patient did not show for appointment (n=19), incorrect tumor site recorded (n=12), duplication of patients (n=4), and inability to access CAIS notes (n=3), resulting in 156 patients’ charts reviewed. • Fraser Valley Cancer Centre consulted one-half as many Lymphoma patients compared to other centers who consulted similar numbers (Table 1). • Most were diagnosed with Non-Hodgkin’s Lymphoma within the past two years and had one or fewer co-morbidities. Twenty patients (13%) were diagnosed with a Lymphoma in the Head and Neck or Gastrointestinal area and 10% had an additional cancer diagnosis (Table 1). • Approximately 70% of the charts either did not have a Nutrition Screening Tool score recorded or the Nutrition Referral Form was not scanned in CAIS to access the score (Table 2). Of those that did have a score, 10% were <4, 10% between 5-8, and 10% were >9. • More than two-thirds of the patients were seen by a dietitian within 2 weeks of referral. Of note though, this information was missing from half of the charts reviewed (Table 4). • More than half the patients (63%) were receiving treatment when seen by the dietitian while (19%) were pre-treatment (Table 4). • Ninety percent of the patients were outpatients with two-thirds of the consults conducted in-person versus by telephone, 30% had also consulted Patient and Family Counseling while only 10% were referred to Community Home Care services (Table 4). • Nutritional indicators showed that BMI was normal or high in 65% of patients even though 22% had lost weight at the time of referral (Table 3). • The most common symptoms impeding nutritional intake were anorexia (28%), nausea (13%), dysphagia (12%)and/or taste changes (8%). Interestingly, 66 patients (43%) did not have any symptoms upon referral (Table 2). • Fifty percent of the patients had a PGSGA score of 8 or less and were assessed to be at low to moderate risk of malnutrition. About 20% of the charts did not have a PGSGA score or risk level assessed (Table 3). • Approximately 10% of the patients had deceased within 6 months of the nutrition consult. • The vast majority of patients (90%) had one or less follow up consult (Table 4). • Malnutrition is commonly seen in patients with cancer, especially cancers of the head and neck and gastrointestinal sites (1). There are a number of nutrition screening tools developed to identify patients at high risk of malnutrition (2). • Due to increasing demands on clinical workload, dietitians are being challenged to prioritize their workload and identify patients at risk for malnutrition and continue to provide optimal nutritional care in the oncology setting. • The dietitians at BC Cancer Agency (BCCA) have developed a tool to help identify patients at high risk of malnutrition called the Nutrition Intervention Framework (NIF). It identifies patients by using a number of factors including diagnosis, symptoms, treatment, and social supports. It also helps to screen, triage and assess patients and plan for follow up in a standardized way. • The literature supports the role for nutrition in head and neck and gastrointestinal cancer but there is no information available on the nutritional needs of Lymphoma patients). • There is a need to gather data on the nutritional management of Lymphoma patients to plan and implement the most cost effective and consistent care guidelines). Table 3. Nutrition Assessment Information Table 1. Patient Demographics and Medical History Table 4. Delivery of Nutritional Care Project Purpose • The aim of this study was to identify nutrition related issues for Lymphoma patients and describe current nutritional care at BCCA to support best practice within the Nutrition Intervention Framework. Methods • A retrospective chart review was conducted of all Lymphoma patients referred to BCCA Oncology Nutrition from January 2007 to December 2007. • Ethical approval was received from the BC Cancer Agency/University of British Columbia Behavioural Research Ethical Review Committee. • Patients were identified from the BCCA Information System (CAIS) using a CAIS code of N/PLY. • Data was collected on the following areas: • --Demographic Information (gender, age, cancer centre) • --Medical History (diagnosis, year of diagnosis, co-morbidities, B symptoms, weight loss, and presence of other cancers) • --Nutritional Screening (Nutrition Screening Tool score, number and type of symptoms impeding nutritional intake) • --Nutritional Assessment (Body Mass Index (BMI), Patient Generated Subjective Global Assessment (PGSGA) score, level of risk of malnutrition • --Delivery of Nutritional Care (time lapse between referral and nutrition consult, inpatient/outpatient, number of follow up consults • Results were tabulated using descriptive statistics using NCSS statistical analysis • Limitations • Due to the retrospective, nature of this project, only reported information could be included • Although CAIS is an easy way to access patient related data, the information recorded is not always consistent between clinics and health professionals. Table 2. Criteria for Nutrition Consult Future Directions • Further analysis of the high and low risk Lymphoma patients may provide helpful information to plan and implement the most cost effective and best practice nutrition guidelines. • Results can help identify strengths and weaknesses of charting practices amongst dietitians and between cancer centres for quality assurance practices. References 1. Isenring E, Capra S, Bauer J: Nutrition Intervention is beneficial in oncology outpatientsreceiving radiotherapy to the gastrointestinal and head and neck areas. British Journal of Cancer 2004; 91: 447-452 2. McCallum, PD: Nutrition Screening, Triage and Assessment. In Nutrition in Cancer Treatment. Eureka, CA: Nutrition Dimensions, Inc., 2003. This is the html version of the file http://www.mascc.org/media/16th_presentation_summaries/McCallumcompleteOverview.doc Accessed November 6, 2008 Acknowledgements to all BCCA Registered Dietitians consulting with lymphoma patients.