Download
1 / 28
280 likes | 302 Vues
This study aims to design an intervention to help pregnant women in deprived areas quit smoking by utilizing social support from their social networks. The research includes phases such as rapid literature review, intervention design, and feedback collection. Key findings from the orientation phase suggest gaps in existing theories on social network health behavior change. The study involves consultations with pregnant women, their social network members, academics, and service providers to create an effective intervention strategy.

E N D
Mapping social networks to support smoking cessation in pregnancy Fiona Dobbie, Lesley Sinclair, School of Heath Sciences and Sport, University of Stirling Andrew Radley, NHS Tayside ISMInstituteforSocial Marketing
Content • Background • Aim • Study design • Key findings – orientation phase • Intervention design • Feedback on proposed intervention • Next steps
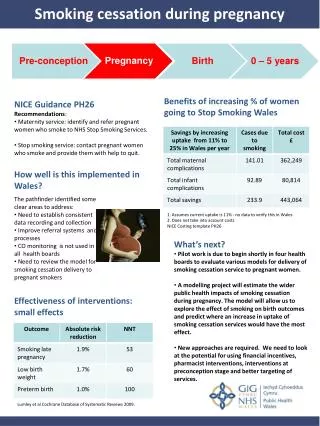
The problem • Smoking in pregnancy is a harmful for both mother and child • Rates of smoking in pregnancy remain high particularly in communities with high levels of social disadvantage • 29% of pregnant women living in the most deprived areas of Scotland were current smokers in comparison with 4.5% living in least deprived area. (Information Service Division Scotland, 2015) • UK Stop Smoking Services support pregnant women to quit. • But, outcomes are poor with only a small proportion of pregnant women who smoke make use of existing services – more innovative approaches required (NICE, 2010)
Social Networks and Health • Our embeddedness in social networks affect our health and behavioural choices (Perkins et al 2015, Hunter et al, 2015) • Attitude and smoking behaviour of partners, family and friends have been identified as barriers to cessation (Hiscock et al 2011, Prady et al 2011). • Studies have shown that reducing the number of smoking friends in a network can help quit attempts (Hitchman, et al, 2014) • Lorencatto et al (2012) emphasised the importance of social support BCTs to aid smoking cessation in pregnancy • Yet, few examples of how this link can be applied.
Study aim To design an intervention to support pregnant women living in deprived areas stop smoking using social support from their social networks.
Study design • Three phases to the study • Orientation – identifying the evidence base, existing theory, clarifying scope and purpose • Intervention design • Feedback on proposed intervention
Study design • Rapid literature review • identity theory and possible models/components of the intervention • Co-creation approach consultation with: • pregnant women (n=7) • members of their social networks (n=8) • academics working in social network research and smoking cessation • Service providers in NHS, Local Authority, and pharmacy staff working in smoking cessation / tobacco control (workshop n=25)
Rapid literature review • Searched for studies using the social network of pregnant women to facilitate any type of HBC during pregnancy and up to 6 weeks postpartum • All type of study design included • Limits • social network defined as friends and family only, not professionals • Articles written in English from 2000 onwards
Summary of paper search and selection process for rapid review
Literature review • Six studies identified where social network members provided social support. • But, long term efficacy was poor and none of them mapped the social network to identify sources of support. • This highlights an important gap in social network health behaviour change theory. • Focus was to identify someone from the social network to offer social support, not how and why they were the most relevant person.
Literature review - existing theory • Who should provide what to whom and when? (Heaney and Israel, 2008) • who – friends and family • what – social support to stop smoking • whom – pregnant women trying to stop smoking • when – during pregnancy and three months post partum • how - ? • To measure effectiveness and access the target group intervention need to be delivered by service providers working with pregnant women (e.g. midwives, health visitors, pharmacists, smoking cessation advisors).
Literature review - existing theory • Heaney and Israel (2008) 5 typologies: • Enhancing existing network ties • Developing new social network linkage • Enhancing networks through the use of natural helpers and community health workers • Enhancing networks through community building and problem solving • Combing strategies
Literature review - existing theory • Valente’s (2012) taxonomy of SN interventions • identify individualsto promote behaviour change • segmentation identifying groups (‘cliques’) who are targets for the intervention • Induction cascading of information e.g. word of mouth, also used as recruitment tool • Alteration seeks to alter the network to change behaviour by adding or deleting nodes
Literature review • Useful but requires mapping andanalysis of social networks - ambitious and resource intensive for service providers • Raised our interest in network visualisation tools (such as concentric circles) and potential hypothesis: • If pregnant women mapped their network and had a better understanding of network structure and resources within it would this influence who they picked to offer social support and how would this affect their smoking cessation attempt?
Concentric circles • Respondent name in centre • Add names of people they feel close to on post it notes • Circles indicate level of closeness • Add detail on • Relationship to them • Age • Employment status • Smoker or non-smoker • Frequency of contact
Concentric circles • Coloured dots added to identify • Who is/has helped them try to quit (yellow dot) • Anyone who is making difficult /made it difficult to quit? (red dot) • Anyone who they would like / would have liked to help them quit but didn’t? (blue dot)
Concentric circles • Maps then used as a tool to enable pregnant women to reflect on: • Strong and weak sources of support • The type of support they receive • Identify ways they can optimise support from their social network • Strategies to manage non supportive members of their social network
Feedback from interviews with PW (N=7) • Support for the idea: • Good to visually see network and think about sources of support • Triggered new insights and ideas • Liked the visual aspect – something they could refer back to and update • Easy to complete and did not take long (around 5 minutes depending on network size)
Feedback from interviews • Points to consider: • Network size varied, common to consist of family members with few friends • Lack of awareness of how social networks could support them - self reliance and will power common approach (one respondent added no dots) • Practicalities of completing the map – language and literacy barriers
Feedback from practitioners • Potential to consolidate existing practice • Gives women insight and lets them make informed choices on network support • Can be used for other health behaviour change • But… • Where does it fit? Who will administer it? • How often would it be used/revisited? • How do you measure impact? (realistic expectations) • Success dependant on confidence of women to engage with her network, but also who delivers it (need staff buy in)
Progress to date Feasibility/Piloting 2017-2020 Pilot 3-arm randomised controlled trial + process evaluation to assess feasibility and acceptability Development 2014-2016 Develop and co-produce intervention theory, website, mobile app, user manual and training resources. Evaluation 1. Assessing effectiveness 2. Understanding change process 3. Assessing cost-effectiveness Implementation 1. Dissemination 2. Surveillance and monitoring 3. Long term follow-up
Research team & advisory group funded by CRUK/BUPA innovation award
Thank you Fiona Dobbie fiona.dobbie@stir.ac.uk ISMInstituteforSocial Marketing