Download
1 / 61
680 likes | 1.02k Vues
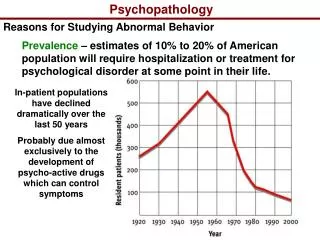
Psychopathology and Treatment. Definition. Psychopathology Clinical term A disorder of the mind that interferes with everyday functioning Insanity Legal term Definition has changed over time

E N D
Definition • Psychopathology • Clinical term • A disorder of the mind that interferes with everyday functioning • Insanity • Legal term • Definition has changed over time • Mental illness or defect decreased the individual’s capacity to appreciate the criminality of their behavior or to conform to the law
Diagnosis • Emil Kraeplin (1883) • First to propose a classification system for mental disorders • Noticed that not all patients with mental illness suffered from the same disorder • Noticed that certain symptoms tended to cluster together as a unique syndrome or disorder
Diagnosis • Categorical vs Dimensional Diagnosis? • Categorical • Set of symptoms that vary together • Must meet minimum threshold (e.g., 4 or more symptoms out of 9), to have the disorder • Dimensional • May involve a set of symptoms • Disorder varies in degree of severity (from non-existent to severe)
Diagnosis • Diagnostic and Statistical Manual of Mental Disorders IV • Categorical diagnostic system • Specifies sets of observable symptoms for each disorder • Specifies criteria for having or not having the diagnosis • Because symptoms of different disorders overlap, gives information for differential diagnosis
Difficulties in Diagnosis • Rosenhan (1973) • 8 participants (pseudo-patients) approached 12 different psychiatric hospitals • All reported hearing voices saying “thud,” “empty,” and “hollow” • Reported no history of psychiatric problems • Reported no other symptoms • All other information about past history was accurate • Once in the hospital, stopped reporting symptom and behaved normally
Difficulties in Diagnosis • All 12 hospitals admitted the pseudo-patients • All pseudo-patients were given the diagnosis of Schizophrenia • Took between 7 and 52 days to be released • All released with a diagnosis of Schizophrenia in Remission • None of staff, but some of the patients, realized that the pseudo-patients were “sane”
Determining Risk • Risk for Self-Harm or Harm of Others • Mental health professionals have legal responsibility to breach confidentiality if they determine that a patient is at risk for harming him/herself or someone else • E.g., Tarasoff Case • Problem determining potential for harm is difficult
Biological/Genetic Brain structure or neuronal defect Inherited predisposition Psychological Faulty defense mechanisms Social Factors Family Systems Model Sociocultural Model Cognitive Behavioral Classical/operant conditioning Modeling/Vicarious reinforcement Causes of Mental Disorder Treatment is based on the conceptualization of the disorder
Anxiety Disorders • Characterized by the experience of excessive anxiety in the absence of true danger and avoidance behavior • Anxiety is our built-in alarm system developed to warn us of a threat and give us the energy to respond to the threat • Excessive, chronic anxiety without identifiable cause and that leads to avoidance of non-threatening stimuli is abnormal
Anxiety Disorders • Phobic Disorders • Social Phobia • Specific Phobias • Generalized Anxiety Disorder • Panic Disorder • With or without agoraphobia • Obsessive Compulsive Disorder • Post-Traumatic Stress Disorder
Symptoms • Panic Disorder • Attacks of terror that are sudden, overwhelming, and unexpected • Did not follow situation that naturally elicits anxiety or in which the individual was the focus of other’s attention • Involves fear of dying, of going crazy, or losing control • With Agoraphobia • Fear of situations where escape might be difficult or embarrassing or where help may be unavailable in the event of an attack • Individual avoids such situations, goes only if accompanied, or endures with significant discomfort
Causes • Biological/Genetic • Locus coeruleus is the area of the brain that perceives novelty serves as an alarm system • Abnormalities of the locus coeruleus result in increased arousal of the central nervous system • Increased arousal of CNS increased sensitivity to internal and external cues signaling threat
Causes • Cognitive Behavioral • Symptoms of anxiety and panic are similar to symptoms associated with heart attack • Panic-prone people monitor bodily sensations for symptoms that might signal an attack • Presence of symptoms result in life-threatening cognitions (catastrophizing) • Increased focus on bodily sensations + catastrophizing spiking of anxiety or panic
Causes W. W. Norton
Causes • Agoraphobia results from negative reinforcement • Individuals are fearful of having another panic attack • Going to places where escape might be difficult or where it would be embarrassing to have an attack increased anxiety • Panic disordered individuals avoid such places • Avoidance avoidance of fear/anxiety increased avoidance
Treatment Panic Disorder with Agoraphobia
Medication • Anxiolytic medications or tranquilizers • Benzodiazepines (e.g., Valium; Klonapin) • Used for short-term treatment of anxiety • Reduce anxiety and promote relaxation • High degree of addiction potential • Selective Serotonin Reuptake Inhibitors (SSRI) • Primarily for the treatment of depression • Appear to have anxiolytic properties • Can be used for long-term • Though not addictive, can have unpleasant side effects
Behavioral Therapy • Cognitive Behavioral Therapy • Education about biological and learning bases of panic • Cognitive Restructuring • Identifying anxiety-producing thoughts • Challenging thoughts with accurate information • Substituting calming and empowering thoughts for anxiety-producing thoughts
Behavioral Therapy • Cognitive Behavioral Therapy • Relaxation training • Diaphragmatic breathing • Progressive muscle relaxation • Systematic desensitization • Imaginal exposure • In vivo exposure
Behavioral Therapy • Systematic Desensitization • Develop fear hierarchy • Expose patient to feared stimuli on hierarchy • Start with a low-fear stimulus • Continue to expose to low-fear stimulus until fear extinguishes • Move to slightly more feared stimulus only after lower-feared stimulus is mastered
Mood Disorders • Mood disorders reflect extreme emotions that affect our ability to function and perform everyday activities
Mood Disorders • Depressive Disorders (AKA unipolar depression) pervasive feelings of sadness • Major Depression • Dysthymia • Bipolar Disorders radical fluctuations in mood from sad to elated or irritable • Bipolar I Major Depression & Mania • Bipolar II Major Depression & Hypomania • Cyclothymia Dysthymia & Hypomania
Symptoms • Depressed mood most of the day, nearly every day • Loss of interest/ pleasure in previously enjoyed activities • Significant weight loss or gain (> 5% of body weight) • Insomnia/hypersomnia • Psychomotor agitation or retardation • Fatigue or loss of energy • Feelings of worthlessness or guilt • Impaired thinking/concentration • Recurrent thoughts of death or of suicide
Causes • Genetic • Twin, family, and adoption studies suggest a genetic component for depression • Identical twins 4 X more likely to be concordant for depression than Fraternal twins • Biological • Low levels of norepinephrine depression • Low levels of serotonin depression
Causes • Biological (continued) • Circadian rhythms, particularly patterns of sleeping and waking, are associated with depression • Seasonal Affective Disorder • As amount of daylight decreases, level of depression increases
Causes • Social/Environmental • More stressful events greater likelihood of developing depression • Having a close friendship mitigates against the impact of stressful life events
Causes • Cognitive (A.T. Beck) • Cognitive Triad • Depressed people think about themselves, their situation, and the future in a negative manner • Attributions • Failures/misfortunes = (internal causes) personal defects • Successes = (external causes) luck • Errors in Logic • Overgeneralizing based on single events • Magnifying the seriousness of events • Taking responsibility for bad events
Causes • Learned Helplessness (Seligman) • People view themselves as unable to control the negative events in their lives • Attribute negative events to personal defects stable and global • People begin to feel helpless about the ability to make positive changes • Theory based on animal research • Animals placed in aversive situations that they could not escape passive and unresponsive
Treatment Depressive Disorders
Medication • Early Antidepressants • Monoamine Oxidase Inhibitors (MAOI) • Effective for treating depression • Highly toxic • Tricyclic antidepressants • Effective for treating depression • Cause weight gain, sedation, sweating, constipation, heart palpitations, and dry mouth
Medication • Modern Antidepressants • Selective Serotonin Reuptake Inhibitors (SSRIs) • e.g., Prozac, Lexapro, Paxil • Increase serotonin levels by blocking reuptake • Some also have norepinephrine effects • Also effective for treating anxiety • Atypical Antidepressants • Bupropion fewer side effects than other antidepressants (no sexual side effects)
Behavioral Therapies • Cognitive Therapy • People are depressed because of negative beliefs about themselves, their situation and the future • Therapy focuses on helping clients • Recognize when they are thinking negatively • Identify the negative thoughts/beliefs • Challenge the beliefs with more positive and adaptive thoughts and/or behavioral experiments
Psychotic Disorders • Psychotic disorders are characterized by disturbances in thoughts, perceptions, consciousness, and emotions • These disturbances lead to impaired social, personal, and/or occupational functioning
Symptoms • Positive Symptoms (excesses) • Delusions false personal beliefs based on incorrect inferences about reality • Hallucinations false sensory perceptions that are experienced w/o an external source • Loosening of associations shift rapidly from one topic to another • Negative Symptoms (deficits) • Socially isolated and withdrawn • Fail to express emotion; speech is monotonic
Treatment Schizophrenia
Medication • Haldol (Haloperidal) • Reduces positive but not negative symptoms • Tardive Dyskinesia • involuntary movements of the lips, tongue, face, legs, or other body part • Irreversible once present (some medications control these symptoms) • Clozapine • Reduces both positive and negative symptoms; Works for unremitting schizophrenia • Side Effects • Seizures, heart arrythmias, weight gain, • Fatal reduction in WBC frequent blood tests required