Flexible Sigmoidoscopy
Flexible Sigmoidoscopy.

Flexible Sigmoidoscopy
E N D
Presentation Transcript
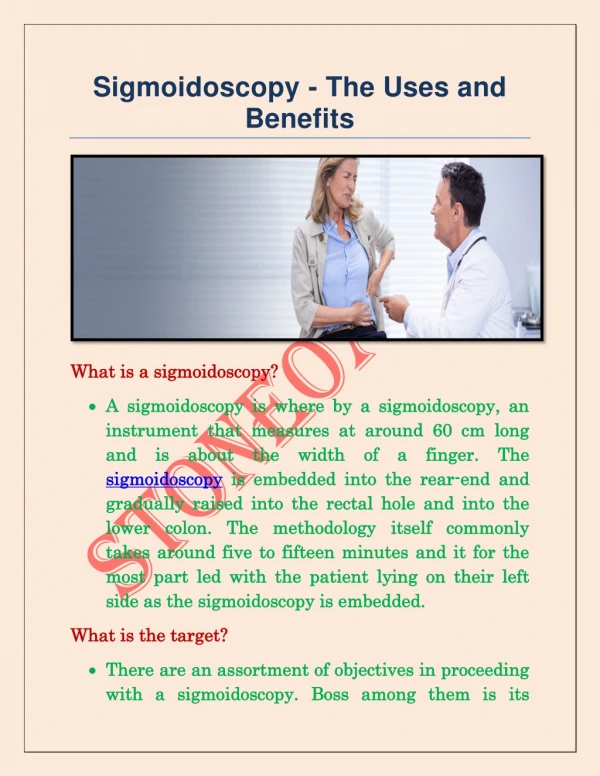
minimally invasive diagnostic medical procedure used to assess the interior surfaces of an organ by inserting a tube into the body. The instrument may have a rigid or flexible tube and not only provide an image for visual inspection and photography, but also enable taking biopsies and retrieval of foreign objects. Endoscopy is the vehicle for minimally invasive surgery. endoscopy:
minimally invasive endoscopic examination of the large colon and the distal part of the small bowel with a CCD camera or a fiber optic camera on a flexible tube passed through the anus. It may provide a visual diagnosis (e.g. ulceration, polyps) and grants the opportunity for biopsy or removal of suspected lesions. Virtual colonoscopy, Furthermore, virtual colonoscopy does not allow for therapeutic maneuvers such as polyp/tumor removal or biopsy nor visualization of lesions smaller than 5 millimeters. colonoscopy:
If a growth or polyp is detected using CT colonography, a standard colonoscopy would still need to be performed. Colonoscopy can remove polyps smaller than one millimeter. Once polyps are removed, they can be studied with the aid of a microscope to determine if they are precancerous or not. Colonoscopy is similar but not the same as sigmoidoscopy.
related to which parts of the colon each can examine. Sigmoidoscopy allows doctors to view only the final two feet of the colon, while colonoscopy allows an examination of the entire colon, which measures four to five feet in length. Often a sigmoidoscopy is used as a screening procedure for a full colonoscopy. The difference between colonoscopy and sigmoidoscopy:-
150,000 cases per year. 50,000 deaths annually. #2 cause of cancer mortality in non-smoking males and females. Colon Cancer
Good evidence that periodic fecal occult blood testing (FOBT) reduces mortality from colorectal cancer and fair evidence that sigmoidoscopy alone or in combination with FOBT reduces mortality. Screening Recommendations
16% of colorectal cancers prevented with FOBT. 34% of colorectal cancers prevented with flex able sigmoidoscopy. 75% prevented with colonoscopy. Colonoscopy q 10 years was more cost-effective than flex sigs q 5-10 (LOE:?). More Evidence
Mostly for screening. Should consider colonoscopy if: previous polyps, family history of colon cancer, rectal bleeding, hemoccult positive stools, change in bowel habits, protracted diarrhea, surveillance in UC/Crohn’s, anemia, unexplained wt. Loss/fevers, abdominal pain. Indications
ABSOLUTE • Acute, severe cardiopulmonary disease. • Inadequate bowel preparation. • Active diverticulitis • Acute abdomen. • History of SBE or prosthetic valves with no prophylaxis. • Marked bleeding dyscrasia. Contraindications
RELATIVE • Recent abdominal surgery (bowel or pelvic). • Active infection • Pregnancy. Contraindications
Light source Suction apparatus Biopsy forceps K-Y Jelly 4X4 inch gauze pads Non-sterile gloves Water container (for suction) Additional Equipment
Video unit and monitor Anoscope Basin of water Formalin jars Disinfecting cleaner More equipment
Bowel perforation (1/10000) Bleeding (increased risk with biopsy) Abdominal distention and pain Infection (SBE, infection from another patient.) Vasovagal symptoms Missed disease Complications
Watch out for patients with previous bowel or pelvic surgery, irradiation, or diverticulosis. Caution with blind advancement (only limited distances). Increased Complications
Signed informed consent 2 fleets enemas (one 90 minutes prior, and one 30 minutes) before procedure Clear liquids after evening meal Take laxative if chronic constipation Take normal medications (caution with diabetics) Patient Preparation
Beverages: carbonated, coffee, kool-aid (avoid red), tea. Desserts: Jello, clear popsicles Fruit: Apple juice, cranberry juice, grape juice Soups: Beef bouillon, clear broth Sweets: hard candy, sugar. Clear Liquid Diet
Patient placed in left lateral decubitus position Rectal examination first Lubrication is key, don’t smear the lens Either directly insert scope, or flex index finger behind the scope. Hold scope in left hand, use thumb for up and down, use right hand for right-left (or can also use thumb). The Procedure
Insert scope 7-15cm, insufflate and/or withdraw to visualize lumen Normal rectal mucosa is a nonfriable, vascular network. Proctitis produces an erythematous, friable mucosa, often with bleeding. Semilunar valves of Houston appear as sharp edges protruding into the lumen (there are 3) with shadows noted behind them. Rectum
Ulcerative colitis will produce erythema, friability, and mucosal bleeding. Rectum
Redundant folds, hard to visualize lumen May have to: insufflate, extensive turning, torquing, accordionization, or dithering Avoid bowing out. Sigmoid
FIGURE 1.Hooking and straightening technique used to pass through a tortuous sigmoid colon. (A) The scope is inserted to the angled sigmoid. (B) The scope tip is turned to a sharp angle, and the sigmoid is hooked as the scope is withdrawn. (C) The sigmoid is straightened as the scope is withdrawn. The scope can then be inserted through to the descending colon. Techniques
FIGURE 2.Paradoxic insertion. (A) The scope is bowing out the sigmoid colon, which has a mobile mesenteric attachment. (B) Paradoxic insertion describes the insertion of the tube without advancement of the scope tip. Paradoxic insertion can be very uncomfortable for the patient. Other Techniques
Long, straight tube with concentric haustrae. Vascularity is random, reticular. Polyps can either be mound-like (sessile) or on a long stalk (pedunculated). Don’t mistake suction polyps or mucous for polyps!! Descending Colon
Accomplished by turning inner knob all the way “up” and outer knob all the way “right” while gently inserting and rotating 180 degrees. Make sure you are in rectum, and not to far from internal sphincter. The Final Step-Retroflexion
Suction air out before terminating procedure! Be nice to your patient