Download
1 / 53
570 likes | 989 Vues
Advances in the Screening, Diagnosis, and Treatment of Cervical Disease. Cervical Cancer. Second most common cancer among women worldwide 1

E N D
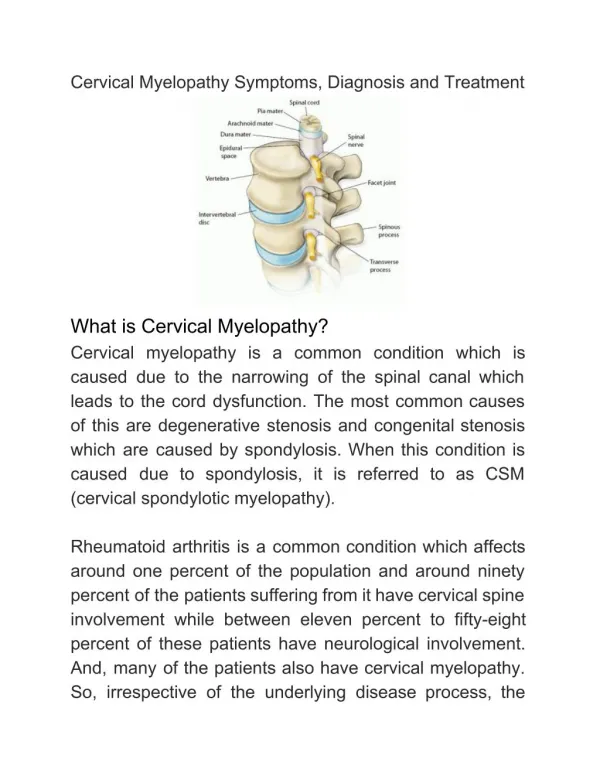
Advances in the Screening, Diagnosis, and Treatment of Cervical Disease
Cervical Cancer • Second most common cancer among women worldwide1 • The American Cancer Society estimates that in 2002, ~13,000 new cases of invasive cervical cancer will be diagnosed in the United States, with about 4,100 deaths2 . In 2001, the estimates were ~ 12,900 cases and 4,500 deaths. • 75% decreased incidence and 73% decreased mortality since Pap screening began in 1949 • However, cervical cancer mortality has not declined in the US since the 1980s 3 1. Walboomers et al. J Pathol. 1999;189:12-19. 2.American Cancer Society, Cancer Facts & Figures 2002. 3. Chu KC et al. Cancer. 1999;86:157-169.
20,000 15,000 10,000 5,000 1975 1980 1985 1990 1995 1970 U.S. Trends in Cervical Cancer Morbidity and Mortality Number of Cases Year Source: National Cancer Institute’s Surveillance, Epidemiology and End Results (SEER) data, American Cancer Society 2001.
0.30 0.25 0.20 0.15 0.10 0.05 0 1930 1940 1950 1960 Year of Birth SEER Trends in North American Incidence of Cervical Adenocarcinoma Cumulative Rate per 1000 Women Black, USA White, USA Canada Hispanic, USA Source: Vizcaino AP et al. Int J Cancer.1998;75:536-545.
Risk Factors Associated With Precancerous Changes and Cancer of the Cervix • Human papillomavirus (HPV) infection • Sexual activity: multiple partners; begun at an early age • Parity • Human immunodeficiency virus (HIV) • Immunosuppressed status • Smoking • History of other sexually transmitted diseases –e.g., Herpes simplex, Chlamydia, bacterial vaginosis • Oral contraceptive use • Low socioeconomic status • Poor diet–e.g., vitamin deficiency • Alcoholism
Cervical Epithelium Showing Progressive Degrees of Dysplasia and Neoplasia LSIL HSIL Koilocytosis CIN1 CIN2 CIN3 Basement membrane Normal Mild Moderate Severe Carcinoma squamous in situ epithelium Dysplasia
Biopsy Regress Persist Progress Progress Result to CIS to Invasion CIN1 57% 32% 11% 1% CIN2 43% 35% 22% 5% CIN3 32% <56% -- >12% Natural History of Cervical Lesions Source: ÖstÖr AG. Int J Gynecol Pathol. 1993;12(2):186-192.
Pap Regress Progress to/ Progress to Diagnosis to Normal Persist as HSIL InvasiveCancer (95% CI) in 24 months in 24 months (95% CI)(95% CI) ASCUS 68.19% (57.51, 78.86) 7.13% (0.8, 13.5) 0.25% (0, 2.25) LSIL 47.39% (35.92, 58.86) 20.81% (6.08, 35.55) 0.15% (0, 0.71) HSIL 35.03% (16.57, 53.49) 23.37% (12.82, 32.92) 1.44% (0, 3.95) Natural History of Cervical Lesions Source: Melnikow J et al. Obstet Gynecol. 1998;92(4Pt2):727-735.
Grade of Dysplasia Within 2 years Within 5 years Within 10 years Progression Mild to moderate or worse 11.1% 20.4% 28.8% Mild to severe or worse 2.1% 5.5% 9.9% Moderate to severe or worse 16.3% 25.1% 32.0% Regression Mild to first normal Pap 44.3% 74.0% 87.7% Moderate to first normal Pap 33.0% 63.1% 82.9% Mild to second normal Pap 8.7% 39.1% 62.2% Moderate to second normal Pap 6.9% 29.0% 53.7% Progression and Regression of Cervical Lesions Source: Holowaty P et al. J Natl Cancer Inst. 1999;91(3):252-258.
Diagnosis Mean Patient Predominant Second Most Age (Years) Patient Status Prevalent Patient Status Carcinoma56.4Postmenopausal Premenopausal (61.9%)(32.4%) HSIL 33.8 Premenopausal Postmenopausal (72.2%) (10.7%) LSIL 30.8 Premenopausal Pregnant (74.4%) (10.2%) Glandular 48.2 Premenopausal Postmenopausal Intraepithelial (50.3%) (38.5%) Lesion Mean Age at Diagnosis of Cervical Lesions Source: Jones BA et al. Arch Pathol Lab Med. 2000;124:665-671.
Cervical Cancer Screening Guidelines:American Cancer Society • All women should have yearly Pap smears starting at age 18 or when they begin having sex, whichever occurs first • The doctor may decide to do the test less often if a woman has had 3 normal tests in a row • If a hysterectomy was done for cancer, more frequent Pap tests may be recommended • Women who have had their uterus removed and those past menopause still need to have regular Pap tests
Bethesda System 2001 Specimen Type:Indicate conventional Pap smear vs. liquid-based vs. other Specimen Adequacy • Satisfactory for evaluation (describe presence or absence of endocervical/transformation zone component and any other quality indicators--e.g., partially obscuring blood, inflammation, etc.) • Unsatisfactory for evaluation (specify reason) • Specimen rejected/not processed (specify reason) • Specimen processed and examined, but unsatisfactory for evaluation of epithelial abnormality because of (specify reason)
Bethesda System 2001(continued) General Categorization (optional) • Negative for intraepithelial lesion or malignancy • Epithelial cell abnormality: See interpretation/result (specify “squamous” or “glandular” as appropriate) • Other: See interpretation/result (e.g., endometrial cells in a woman 40 years of age) Automated Review:If case examined by automated device, specify device and result Ancillary Testing:Provide a brief description of the test methods and report the result so that it is easily understood by the clinician
Bethesda System 2001(continued) Interpretation/Result • Negative for Intraepithelial Lesion or Malignancy (when there is no cellular evidence of neoplasia, state this in the General Categorization above and/or in the Interpretation/Result section of the report, whether or not there are organisms or other non-neoplastic findings) Organisms • Trichomonas vaginalis • Fungal organisms morphologically consistent with Candida spp • Shift in flora suggestive of bacterial vaginosis • Bacteria morphologically consistent with Actinomyces spp. • Cellular changes consistent with Herpes simplex virus Other Non-Neoplastic Findings (optional to report; list not inclusive): • Reactive cellular changes associated with • Inflammation (includes typical repair) • Radiation • Intrauterine contraceptive device (IUD) • Glandular cells status post hysterectomy • Atrophy
Bethesda System 2001(continued) • Other (list not inclusive) • Endometrial cells (in a woman 40 years of age) (specify if ‘negative for squamous epithelial lesion’) • Epithelial Cell Abnormalities • Squamous Cell • Atypical squamous cells • Of undetermined significance (ASC-US) • Cannot exclude HSIL (ASC-H) • Low-grade squamous intraepithelial lesion (LSIL) • Encompassing: HPV/mild dysplasia/CIN1 • High-grade squamous intraepithelial lesion (HSIL) • Encompassing: moderate and severe dysplasia, CIS/CIN2 and CIN3 • With features suspicious for invasion (if invasion suspected) • Squamous cell carcinoma
Bethesda System 2001(continued) • Glandular Cell • Atypical • Endocervical cells (NOS* or specify in comments) • Endometrial cells (NOS or specify in comments) • Glandular cells (NOS or specify in comments) • Atypical • Endocervical cells, favor neoplastic • Glandular cells, favor neoplastic • Endocervical adenocarcinoma in situ • Adenocarcinoma • Endocervical • Endometrial • Extra uterine • NOS • Other Malignant Neoplasms: (specify) * NOS = Not otherwise specified
Bethesda System 2001(continued) Educational Notes and Suggestions:(optional) Suggestions should be concise and consistent with clinical follow-up guidelines published by professional organizations (references to relevant publications may be included)
Bethesda 2001 Changes • Satisfactory: Liquid-based—minimum 5,000 epithelial cells; presence of epithelial cell abnormality • “SBLB” eliminated • Unsatisfactory: specimen rejected/not processed; or specimen processed/examined, but unsatisfactory because of (specify reason) • WNL and BCC are now Negative for Intraepithelial Lesions or Malignancy; includes BCC (e.g., organisms and reactive changes) as descriptor only • The multiple subcategories of ASCUS have been reduced to ASC-US or ASC-H, with no other modifiers • The subcategories of AGUS (now AGC) have been expanded to allow for a more descriptive diagnosis of glandular abnormalities; AIS is now a distinct subcategory
The Bethesda System 2001 • LSIL = HPV / mild dysplasia / CIN1 • HSIL = moderate and severe dysplasia / CIS / CIN2 and CIN3 • ASCUS = ASC-US (undetermined significance) or ASC-H (cannot exclude HSIL)
Annual Number of Women with Abnormal Pap Results in the US Cancers 12,800 300,000 HSIL LSIL 1.25 million AGC 180,000-300,000 ASC 2- 3 million Source: J. Thomas Cox, with permission.
Sensitivity of the Pap Smear Mean Sensitivity of Conventional Pap Smear (%), 95% CI 1. Agency for Health Care Policy and Research (AHCPR). Evaluation of Cervical Cytology. 1999. 2. Fahey MT et al. Am J Epidemiol. 1995;141:680-689.
Two Types of Screening Conventional Pap Smear • Cervical cell sample manually “smeared” onto slide for screening Liquid-Based • Cervical cell sample put into liquid medium for suspension before automated thin layer/monolayer slide preparation • ThinPrep® 2000 System • SurePathTM (formerly AutoCyte® PREP)
Conventional Pap Smear * From ThinPrep Sampling Study, Hutchinson 1994 Overcoming the Inherent Limitations of the Conventional Pap Smear Liquid-based Cytology* • Majority of cells not captured • Non-representative transfer of cells • Clumping and overlapping of cells • Obscuring material • Virtually all cells of sample are collected • Randomized, representative transfer of cells • Even distribution of cells • Minimizes obscuring material
Overview of Liquid-Based Cytology:FDA Labeling ThinPrep® Pap Test SurePath™ • Used as a replacement for the conventional Pap smear • Specimen quality is significantly improved over that of the conventional Pap smear in a variety of patient populations • Significantly more effective than the conventional Pap smear for the detection of low-grade and more severe lesions in a variety of patient populations • Specimens should be collected using a broom-type or endocervical brush/spatula combination collection device • Increased HSIL+ detection by 59.7% (data from a multi-site, historical control study) • Approved as a specimen medium for HPV DNA testing using Digene Hybrid Capture® 2, as well as for chlamydia and gonorrhea screening • Used as a replacement for the conventional Pap smear • Significantly fewer Unsatisfactory and SBLB cases as compared to the conventional Pap smear • Provides similar results to the conventional Pap smear (data from a prospective split-sample comparison in a variety of patient populations and laboratory settings) • Specimens should be collected using a broom-type sampling device ThinPrep® Pap Test Package Insert, Cytyc Corporation AutoCyte PREPTM SYSTEM package insert (now SurePathTM), TriPath Imaging, Inc.
HSIL+ Clinical Outcomes Trial • Direct-to-vial study to evaluate ThinPrep 2000 vs. conventional Pap for the detection of high-grade squamous and more severe lesions (HSIL+) • 10 metropolitan academic hospitals, two groups of subjects per site: • Routine screening population • Referred for colposcopy • ThinPrep specimens (n = 10,226) collected prospectively compared to historical control cohort (n = 20,917) • These sites demonstrated a 59.7% (p <0.001) increase in detection of HSIL+ lesions for ThinPrep specimens
HPV Testing – Essential Facts • HPV is the major etiologic agent for cervical cancer • HPV detection is associated with an increased risk of high-grade CIN • Essentially all women with CIN3 have detectable HPV DNA • Persistent infection with high-risk HPV is necessary for development and maintenance of CIN3 • HPV testinghelps to clarify ambiguous cytology results and identifies persistent infection in women over 30
HPV Risk Types Hybrid Capture®2 (HC II) HPV DNA Test uses two RNA Probe cocktails to differentiate between carcinogenic and low-risk HPV types: Low-risk 6 11 42 43 44 High-risk 16 18 31 33 35 39 45 51 52 56 58 59 68
30 30 25 25 20 20 15 15 10 10 5 5 0 0 15-19 20-24 25-29 30-34 35-39 40-44 45-49 50-54 HPV Prevalence and Cervical Cancer - Incidence by Age1,2 Cancer incidence per 100,000 HPV Prevalence (%) Age (Years) 1. Sellors et al. CMAJ. 2000;163:503. 2. Ries et al. Surveillance, Epidemiology and End Results (SEER) Cancer Stats NCI, 1973-1997. 2000.
Pap Smear Incidence Incidence Incidence Cytology (Manos et al) (Chhieng et al) (Stoler) HSIL 0.3% SIL+ 2.5% 0.51% LSIL 0.9% -- 1.97% ASCUS 3.5% 5.7% 2.8% AGUS 0.5% 0.5% -- Incidence of Atypical Findings 1. Manos MM, Kinney WK, Hurley LB, et al. J Am Med Assoc 1999;281(17):1605-1610. 2. Chhieng DC, Elgert PA, Cangiarella JF, et al. Acta Cytol 2000;44(4):557-566. 3. Stoler MH. Mod Pathol 2000;13(3):275-284.
Comparison of HPV Testing and Repeat Pap in the Management of ASCUS Triage Referred to Sensitivity PPV for Strategy Colposcopya for HSIL+ HSIL+ Based on HPV Testb 39.5% 89.2% 15.1% Based on Repeat Pap Resultc 38.9% 76.2% 12.9% • PPV = positive predictive value • Notes: • Prevalence of positive test result in women with ASCUS • Referral to colposcopy based on positive DNA test for high-risk HPV types, from specimen on initial visit • Referral to colposcopy based on repeat Pap test result of ASCUS or more severe Source: Manos et al, JAMA. 1999;281(17):1605-1610.
ALTS Study Design • Randomized trial sponsored by NCI, 1995-2001 • Enrolled 3488 women with community-based ASCUS and 1572 with LSIL results, randomized to three management arms: • Immediate colposcopy • HPV triage • Repeat cytology • Clinical follow-up every 6 months for 2-year period • LSIL arm discontinued due to limited utility of positive test result Source: Solomon D et al. J Natl Cancer Inst. 2001;93:293-299.
Sensitivity for CIN2+ by HC II & Pap by Age Clinical Center Pap 18-22 23-28 29+ Cutpoint %(+) / Sens%(+) / Sens%(+) / Sens HC II 71 / 98 65 / 96 31 / 94 ASCUS+ 66 / 83 63 / 88 50 / 87 Sherman M, Schiffman M, Cox JT. J Nat Cancer Inst. 2001
HPV HPV Total risk Positive Negative ASCUS Cox 17% 0.74% 6.9% 1995 (14/81) (1/136) (15/217) Manos 15% 1.2% 6.4% 1999 (45/300) (6/498) (51/801) ALTS 20.1% 1.1% 11.9% 2001 (136/651) (6/541) (142/1192) Total 17.9% 1.1% 9.4% (195/1087) (13/1175) (208/2210) Risk of CIN 2/3+ for ASC referralBased on HPV status at enrollment Cox JT, et al. Am J Obstet Gynecol. 1995 Mar;172(3):946-54.Solomon D, et al. J Natl Cancer Inst. 2001;93:293-299. Manos et al, JAMA. 1999;281(17):1605-1610.
Primary Findings: ALTS Management Sensitivity %* Referral % PPV % NPV % Modality Colposcopy 100 100 11 100 HPV 96 56 20 99 Cytology ASC-US+ 85 59 17 96 Cytology LSIL+ 59 26 26 94 Cytology HSIL+ 35 8 58 92 PPV = positive predictive value; NPV = negative predictive value *For detection of (CIN2+) Adapted from table 5, Solomon D et al. J Natl Cancer Inst. 2001;93:293-299.
ASCCP Consensus Guidelines for the Management of Abnormal Cervical Cytology and Cervical Cancer Precursors • Held in Sept. 2001, NCI campus, 29 national and international organizations including ACS, NCI, CDC, ACOG, all the major cytopathology organizations, etc. • The guidelines were all evidence-based (to the limits of the literature) • They were placed on the Consensus Guidelines Website twice during the 6 months prior to the conference for public comment and appropriate revisions were made • All of the guidelines were approved by a majority and most were approved by 70-90%
AGC Findings from 306 LaboratoriesParticipating in CAP Survey 2000 AGC Rate SIL AIS CA 0.3% 40% 5.8% 5.5% Jones BA, Novis DA. Follow-up of abnormal cervical cytology: a College of American Pathologists Q Probes Study of 16,132 cases from 306 laboratories. Arch Pathol Lab Med. 2000;124:672-681. (1-C)
Qualifier Any High-grade Lesion High-grade Glandular Lesion Only AGUS reactive 5 – 39% 1 – 8% AGUS NOS 9 – 41% 0 – 15% AGUS neoplastic 27 – 96% 10 – 93% Clinical Significance of an AGC Pap Source: Richart et al. Contemp Ob Gyn. 2001; 46:15-17,25-28,30-32,35-43.
Management of LSIL: Special Circumstances • Mod: Abnormal Pap-fig 6
Management of HSIL • Mod: Abnormal Pap-fig 8
Candidates for Ablative or Excisional Therapy • Patients who are suitable for ablative therapy have: • The entire transformation zone visualized (satisfactory colposcopy) • No suggestion of microinvasive or invasive disease • No suspicion of glandular disease • Corresponding cytology and histology • Patients in whom excisional treatment is mandatory have: • Unsatisfactory colposcopy • Suspicion of invasion or glandular abnormality
Excisional Techniques Conization • A cone of tissue is excised for further examination and/or to remove a lesion • The tissue is usually stained with iodine (Lugol’s or Schiller’s solution) to demarcate the area of resection • Cold Knife Cone • The use of a scalpel or “cold knife cone” since no electrosurgical current is used • Laser Conization • The use of a laser for excision of a cone of tissue • May be complicated by burn artifacts • LEEP (Loop Electrosurgical Excision Procedure) • The use of a thin electric wire loop, which may have cutting and cautery currents • Different sizes of loop and cautery tip available • May be complicated by burn artifacts
Ablative Techniques Cryotherapy • The use of a probe containing carbon dioxide or nitrous oxide to freeze the entire transformation zone and area of the lesion • Different sizes of probe available Laser Vaporization Therapy • The use of a laser to vaporize the transformation zone containing the lesion • Requires suction to remove smoke • Different power levels are available
Cervical Cancer: FIGO Nomenclature Stage 0: Carcinoma in situ, cervical intraepithelial neoplasia Grade III Stage I: The carcinoma is strictly confined to the cervix (extension to the corpus would be disregarded). Stage II: Cervical carcinoma invades beyond the uterus, but not to the pelvic wall or lower third of the vagina. Stage III: The carcinoma has extended to the pelvic wall. On rectal examination, there is no cancer-free space between the tumor and the pelvic wall. The tumor involves the lower third of the vagina. All cases with hydronephrosis or non- functioning kidney are included, unless they are known to be due to other causes. Stage IV: The carcinoma has extended beyond the true pelvis, or has involved (biopsy-proven) the mucosa of the bladder or rectum. A bullous oedema, as such, does not permit a case to be allotted to Stage IV.