Download
1 / 43
430 likes | 608 Vues
Getting Knowledge into Action to Deliver the Future for Scotland’s Healthcare. “Knowing is not enough; we must apply. Willing is not enough; we must do.” - Goethe. Delivering the Future Residential Session 17 th January 2012. Overview.

E N D
Getting Knowledge into Action to Deliver the Future for Scotland’s Healthcare “Knowing is not enough; we must apply. Willing is not enough; we must do.” - Goethe Delivering the Future Residential Session 17th January 2012
Overview A new knowledge paradigm at the heart of transformational leadership. Practical tools for continuous co-creation of knowledge by combining content, communication, collaboration. 3. Discussion - knowledge into action supporting your clinical leadership role. 4. Where we are now – your role in leading knowledge into action….
Crossing the Quality Chasm The gulf between what we know is good quality care and what is the norm in practice.
Too much information…. “Seventy-Five Trials and Eleven Systematic Reviews a Day: How Will We Ever Keep Up?” Bastian, H., Glasziou, P., Chalmers, I. PLOS-Medicine, 2010 Clinician would need to read at least 20 articles per day, 365 days per year, to keep up with new developments in their field. Shaneyfelt, T. et al JAMA 2001
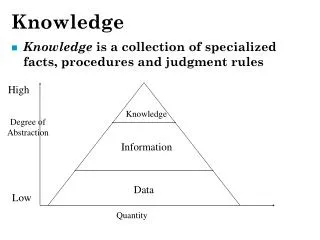
“The NHS is….. not good at capturing, using and sharing information. Lots of data, a lot less information and even less knowledge, and that's bad for patients and their families, it's bad for clinicians, bad for managers, bad for regulators and bad for policy-makers.”Ann Abraham, Parliamentary and Health Service Ombudsman, reporting on Mid-Staffordshire Inquiry.
From Accessing to Applying Knowledge in NHS Scotland Knowing 66 libraries 116 library staff 12 million + resources Doing How much of this gets used in a meaningful way to improve safe, effective, person-centred care?
Knowledge-practice gap 45% defect rate in US healthcare system – patients not receiving care as recommended in the evidence base. (McGlynn et al,2003) 30-40% defect rate in UK healthcare (Grol and Grimshaw, 2003) 17 years to get 14% of research recommendations into practice (Balas et al 2000)
What about care in 2011? NHS Atlas of Variation in Healthcare Percentage of people in the National Diabetes Audit with Type 1 diabetes receiving all nine key care processes Highest value is less than 50%.
Aim:Define a national system for knowledge management and utilisation in order to:* help practitioners to apply knowledge to frontline practice. * align use of knowledge with improving healthcare quality * support practitioners and managers to translate knowledge into better health outcomes, i.e. safe, effective, person-centred, efficient care. Knowledge into Action Review
A new lens for healthcare knowledge Published research – our mainstay, but partial… Evidence only available for 20% of clinical issues; rest is opinion (Williamson 1979, Sackett, 1995 and others). 2. Irreproducibility of research results (Naik, 2011) 3. Overestimation of impact in research studies compared with real-life contexts (Ioannidis, 2011). 4. Limitations in applying research results to individual patients with complex care needs and individual preferences. (Kent, 2007)
Changing the knowledge paradigm Continuously co-produce knowledge through collaboration with teams, patients and carers. Customise knowledge to context Personalise knowledge to individual patient care. Understand, manage and use variation to build the knowledge base. Embed knowledge in clinical workflow
Recognise role of practice and experiential knowledge Need a new knowledge paradigm which constantly generates new knowledge by combining research evidence routine practice data working experience of teams lived experience of individual patients and carers. “Living guidelines” embedded in practice Underpins continuous learning and continuous improvement – research in action.
Example – Intermountain Healthcare Brent James, Morris, Orme, 1998: Created initial protocol for treating ARDS. Placed by bedside as prompt / reminder in clinical workflow. Clinicians encouraged to use as the default but to depart from the protocol when necessary. Reduction in variation through engagement enabled to isolate the aspects of treatment that made a difference. Weekly team meetings to review outcomes and reasons for deviation from protocol – reviewed protocol to reflect reality of practice and patient need. 40% survival rate in ARDS compared with 10% survival as national average. Now extended to more than 50 clinical conditions. Improving quality reduces cost.
Transfer of Knowledge into Quality Patient Care Doing the right thing Clinical Decisions Doing it right Process/System Changes Quality Patient Care Clinical Knowledge (Evidence Based Practice): MEDLINE, Cochrane etc Know-What Experiential Knowledge: Practice, Patient, Context, System Know-How Adapted from: Glasziou, P et al. Can evidence-based medicine and clinical quality improvement learn from each other? 2011. BMJ Qual Saf 20 (suppl 1): i13-i17
Evidence Base What approaches help to get knowledge into action to improve quality of care? Huw Davies and Vicky Ward 2011 Inquiry and synthesis Actionable knowledge Relational knowledge Building organisational culture and capacity Knowledge into Action roles
Examples (1) Inquiry and synthesis Problem definition Expert searches Rapid evidence reviews Capture tacit/experiential knowledge – case studies, stories, social networking Partner with information analysts to combined data and research evidence.
Examples (2) Actionable knowledge Specific evidence expressed as calls to action; designed for use at point of clinical need. Pathways Evidence bundles Checklists Prompts and reminders Decision aids/decision support Mobile apps “Actionable knowledge”
Examples (3) Relational knowledge Communities of practice One to one knowledge transfer (clinical detailing) Champions, opinion leaders Interactive education Social network mapping Social networking and social media tools Patient education and health literacy
Examples (4) Organisational capacity and capability Workforce knowledge management skills Knowledge broker roles Defined knowledge management strategy and policy
Build on KM expertise in:* Evidence search, synthesis, packaging;* Facilitating sharing of knowledge- communities, 1-1 knowledge transfer;* Planned dissemination and uptake* Building workforce capabilities in K2A Knowledge broker roles
Example –Knowledge into Action for Improvement Problem A mental health team leader identifies from readmissions data and complaints a need to improve cross-agency communication in care of schizophrenia patients on discharge from hospital. Aim : Reliable communication for 95 % of patients with schizophrenia on discharge from hospital by June 2012
Know-what He asks the knowledge manager to source and summarise the research evidence on interventions and outcome measures to improve cross-agency communication in care of schizophrenia patients discharged from hospital.
Know-how and know-who: Knowledge management support to help implement new approaches effectively: Sourcing case studies Published research – evaluations of implementation Gathering good practice from communities of practice and interviews with organisations facing similar challenges Sharing stories with staff and service users Peer assist sessions – identifying subject experts to contribute their knowledge
Creating knowledge Knowledge manager and team leader work together to create a checklist for use by NHS, partner agency staff, service users and carers (actionable knowledge). They publish a summary of the new approach and a case study on the community website with links to the relevant evidence and guidelines (knowledge assets).
Discussion Think of a situation where your leadership role calls for you to translate knowledge into action. How could the knowledge into action approaches illustrated help you to improve healthcare quality in this situation?
Knowledge into Action in NHS Scotland Current status and development path “The future is already with us; it’s just not evenly distributed”William Gibson
Overview Current knowledge into action tools and services. National network of knowledge management support. Test of change projects – first steps in implementation.
Actionable Knowledge Validated knowledge - designed for implementation in frontline practice
Actionable Knowledge Services www.knowledge.scot.nhs.uk
Decision Support “plug-in” Point of Care Knowledge
m.decisionsearch.scot.nhs.uk Homepage App Store
Creating actionable knowledge Publication tool – for pathways and SIGN guidelines. Decision support rules – to link with clinical systems.
Example: Sepsis and VTE Aim: Define and Implement Improvements for Management of Sepsis in VTE Knowledge Management Support: Evidence for intervention and implementation Community of practice support Territorial Board and Special Board partnership
Expert evidence search and synthesis HIS and territorial board knowledge managers Problem definition “Know-what” clinical evidence for interventions Cochrane, Medline, EMBASE etc. “Know-how” and “know-who” examples of implementation in US, UK; key contacts.
Community of Practice forSepsis and VTE Share and disseminate knowledge across boundaries of discipline and organisation. Peer support Sharing ideas and learning Combine published knowledge with personal experience Repository Generate new knowledge Translate knowledge into action
Homepage of the community website Collaborative tools Log in with NHS Athens username Search box Library of communities resources Navigation Boxes of functionality managed by the administrators of the website
Tests of change 20 projects 6 special boards, including State Hospital 5 territorial boards K2A areas: Expert search Create and use actionable knowledge– decision support, pathways, bundles etc. Close interaction with clinical and programme teams (social use of knowledge) Coordinated KM teams
Examples Rapid search and synthesis for decision support in clinical settings. Virtual clinical librarian. Knowledge bundle to support perioperative care of diabetes patients Development of knowledge broker role for practice educators. Coordinating knowledge management roles across departments to support alcohol team.
Summing up Knowledge as a dynamic force for transformational change. Build organisational capacity to identify critical knowledge, blend into daily workflow and disseminate to all who need it, as actionable and relational knowledge.
Contacts Ann.wales@nes.scot.nhs.uk Karenritchie@nhs.net Annette.thain@nes.scot.nhs.uk Kevin.rooney@uws.ac.uk
Getting Knowledge into Action to Deliver the Future for Scotland’s Healthcare Delivering the Future Residential Session 17th January 2012 “Knowing is not enough; we must apply. Willing is not enough; we must do.” - Goethe