Download

1 / 171
1.74k likes | 1.8k Vues
Learn about the physiology and anatomy of glaucoma, including aqueous secretion, outflow, and factors influencing intraocular pressure. Explore the pathogenesis and classification of glaucomas for proper diagnosis and treatment.

E N D
Diagnostic and treatment of glaucoma Małgorzata Seredyka-Burduk
IntroductionPhysiology and anatomy Aqueous secretion Active secretion accounts for approximately 80% of aqueous production. The aqueous is secreted by the non-pigmented ciliary epithelium via an active metabolic process that is dependent on number of enzymatic systems.
IntroductionPhysiology and anatomy Aqueous secretion Passive secretion accounts for the remaining 20%. Aqueous is produced by passive processes such as ultrafiltration and diffusion which are dependent on the level of blood pressure in the cilliary capillaries, the plasma oncotic pressure and the level of intraocular pressure.
IntroductionPhysiology and anatomy Aqueousoutflow Aqueushumourleaves the eye by trabeculum. The trabeculum (trabecularmeshwork) is a sieve-likestructure. Aqueous outflow Aqueus humour leaves the eye by trabeculum. The trabeculum (trabecular meshwork) is a sieve-like structure.
IntroductionPhysiology and anatomy The trabeculum consists of three portions: 1. The uveal meshwork (a) is the innermost portion which consists of cord-like meshes that extend from the root of the iris to the Schwalbe’s line. The intertrabecular spaces are relatively large and offer little resistance to the passage of aqueous.
IntroductionPhysiology and anatomy 2. The corneoscleral meshwork (b) forms the larger middle portion which extends from the scleral spur (g) to Schwalbe’s line (c). The meshes are sheet-like and the intertrabecular spaces are smaller than in the uveal meshwork.
IntroductionPhysiology and anatomy 3. The endothelial meshwork is the narrow outer part of the trabeculum which links the corneoscleral meshwork with the endothelium on the inner wall of Schlemm’s canal (d).
IntroductionPhysiology and anatomy Schlemm’s canal is a circumeferential channel bridged by septa. The inner wall of the canal is lined by irregular spindle-shape endothelial cells which contain giant vacuoles. The outer wall of the canal is lined by smooth flat cells and contain the openings of the collector channels.
IntroductionPhysiology and anatomy Aqueous flows from the posterior chamber into the anterior chamber through the pupil and is drained by the two routes: • The trabecular (conventional) route (accounting 90% of aqueous outflow) is through the trabaculum into Schlemm’s canal and episcleral veins.
IntroductionPhysiology and anatomy • The uveoscleral (unconventional) route accounts 10%. The aqueous passes across the cilliary body into the suprachoroidal space and is drained by the circulation in the cilliary body, choroid and sclera. Some aqueous also drains via the iris.
IntroductionPhysiology and anatomy The followingfactorsdetermine IOP: • rate of aqueoussecretion, • resistanceencountered in the outflowchannels, • level of episcleralvenouspressure The normal IOP variesbetween 10mmHg and 21 mmHg. Althoughthereis no absolutecutoff point, 21 mmHgisconsidered the upper limit of normal, and levelsabovethisareviewed with suspicion.
IntroductionPhysiology and anatomy Fluctuations of IOP occur with the time of day, heartbeat, blood pressure level and respiration. Normal eyes have a smaller diurnal fluctuations (<4mmHg) than eyes with glaucoma in which the fluctuation may be 10mmHg or more.
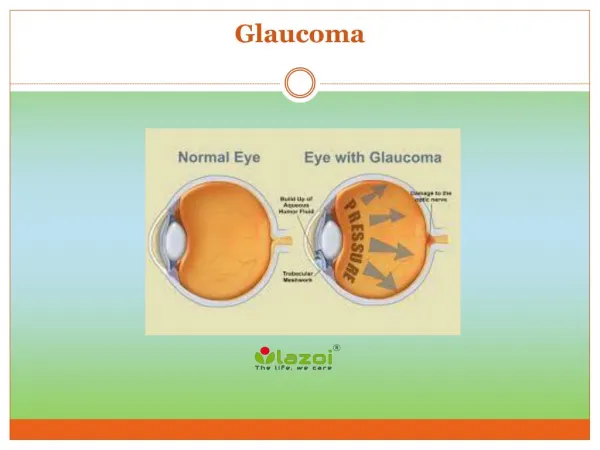
IntroductionPathogenesis of glaucomatousdamage of opticnerve 1. The ischaemic theory postulates that raised IOP causes death of nerve fibres because of too low perfusion pressure (difference between the IOP and the intracapillary pressure). 2. The mechanical theory suggests that elevated IOP directly damages the retinal nerve fibres as they passed through the optic nerve head. It seems likely that both mechanisms play a role in most cases.
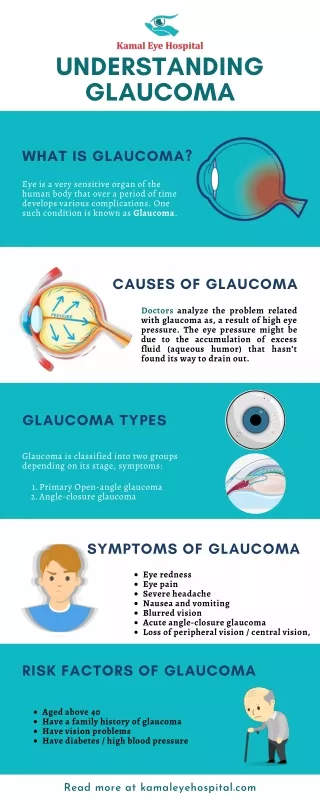
IntroductionClassification of the glaucomas 1. Open-angle glaucomas 2. Angle-closure glaucomas 1. Primary glaucomas (the elevation of IOP is not associated with any other ocular disorder) 2. Secondary glaucomas (an ocular or non-ocular disorder alters aqueous outflow – this results in elevation of IOP).
IntroductionClassification of the glaucomas There are the following secondary open-angle glaucomas: • pre-trabecular (aqueous outflow is obstructed by a membrane covering the trabeculum) • trabecular (the obstruction occurs within the trabeculum itself)
IntroductionClassification of the glaucomas There are the following secondary open-angle glaucomas: • post-trabecular (the trabeculum by itself is normal but aqueous outflow is impaired as a result of elevation of pressure in episcleral veins)
IntroductionClassification of the glaucomas Secondary angle-closure glaucomas are those in which aqueous outflow is impaired by apposition between the peripheral iris and the trabeculum. This may be the result of: • posterior forces which push peripheral iris against the trabeculum • anterior forces which pull the peripheral iris over the trabeculum
IntroductionClassification of the glaucomas In generally, primary open-angle glaucoma (POAG) is most common and accounts for 55% of cases, secondary glaucomas are next (30%), followed by primary angle-closure glaucoma (PACG) – 12% and congenital – 3%.
Methods of examination Tonometry The two main methods of measuring IOP are by applanation (The Goldmann tonometer, The Perkins tonometer, The air-puff, The Pulsair, The Tono-Pen) and indentation (The Schiotz tonometer). Both are based on the principle that the applied force either flattens (applanates) or indents the cornea.
Methods of examination Gonioscopy The main purposes of gonioscopy: • identification of abnormal angle structures • estimation of the width of the chamber angle • visualization of the angle during procedures such us laser trabeculoplasty and goniotomy
Methods of examination The angle of the anterior chamber cannot be visualized directly through an intact cornea because light emitted from angle structures undergoes total internal reflection. A goniolens eliminates this by replacing the cornea/air interface with a new interface which has a refractive index greater than that of the cornea and tears.
Methods of examination The two main types of goniolenses are: 1. indirect (provide a mirror-image view of the opposite angle and can be used only with conjunction with a slitlamp) – the Goldmann goniolens, the Zeiss goniolens
Methods of examination The two main types of goniolenses are: 2. direct (provide a direct view of the angle and is usually used with the patient in the supine position during operations on the angle) – the Koeppe goniolens, the Swan-Jacob goniolens, the Barkan goniolens
Methods of examination The Goldmann goniolens gives an excellent view of the angle structures, stabilizes the globe, is suitable for laser trabeculoplasty. The curvature of the contact surface of the lens is steeper than that of the cornea, so a viscous coupling substance, with the same refractive index as the cornea, that bridges the gap between the cornea and the goniolens is required.
Methods of examination The Zeiss goniolens has four mirrors, so the entire extent of the angle may be visualized with minimal rotation. As the curvature of the contact surface of the lens is flatter than that of the cornea, coupling substance is not required.
Methods of examination The Zeiss goniolens does not stabilize the globe, but if the lens is pushed hard against the cornea, it will distort it and impair visualization of the angle. This will also displace aqueous humour to the periphery of the angle, so that a narrow angle may appear artificially wide. indentation gonioscopy
Methods of examinationIdentification of anglestructuresduringgonioscopy Schwalbe’s line is the most anterior structure appearing as an opaque line. It represents the peripheral termination of Descemet’s membrane and the anterior limit of the trabeculum. In locating Schwalbe’s line is useful the corneal wedge. Using a narrow slit beam, two linear reflections can be seen: one from the external surface of the cornea and its junction with sclera, the other from the internal surface of the cornea. The two reflections meet at Schwalbe’s line which forms the apex of the corneal wedge.
Methods of examinationIdentification of anglestructuresduringgonioscopy The trabeculum has a ground-glass appearance and appears to have a depth. It consists of the two parts: the anterior, non-functional, non-pigmented, lies behind the Schwalbe’s line, has a whitish colour. the posterior, functional, pigmented, lies between the anterior trabeculum and scleral spur, has a greyish-blue colour.
Methods of examinationIdentification of anglestructuresduringgonioscopy Pigmentation of the trabeculum is very rare before puberty. In senile eyes it involves the trabeculum to a variable extend and is most marked inferiorly. Pathological trabecular hyperpigmentation is caused by excessive shedding of pigment from the posterior layer of the iris. In eyes without trabecular pigmentation Schlemm’s canal can occasionally be identified as a slightly darker line deep to the posterior trabeculum.
Methods of examinationIdentification of anglestructuresduringgonioscopy The scleral spur is the most anterior part of the sclera and the site of attachment of the longitudinal muscle of the ciliary body. It appears as a narrow, dense, shiny, whitish band. The scleral spur is the most important landmark because it has relatively consistent appearance in different eyes.
Methods of examinationIdentification of anglestructuresduringgonioscopy The ciliary body stands out just behind the scleral spur as a dull-brown or slate-grey band. Its width depends on the position of the iris insertion and tends to be narrower in hypermetropic eyes and wider in myopic eyes.
Methods of examinationIdentification of anglestructuresduringgonioscopy Iris processes are small extensions of the anterior surface of the iris which are inserted at the level of scleral spur and cover the ciliary body. Iris processes are present in about one-third of normal eyes and are most prominent during childhood and in brown eyes. Iris processes should not be confused with peripheral anterior synechiae, which are adhesions between the iris and the angle structures!
Methods of examinationGrading of anglestructures Its main aims are to evaluate the functional status of the angle, its degree of closure and the risk of future closure.
Methods of examinationGrading of anglestructures In the Shaffer system, an estimation of the angle width is achieved by observing the amount of separation between two imaginary lines, constructed to the inner surface of the trabeculum and the anterior iris surface.
Methods of examinationGrading of anglestructures Grade 4 (35°-45°) is the widest angle characteristic of myopia and aphakia in which the ciliary body can be visualized. It is incapable of closure.
Methods of examinationGrading of anglestructures Grade 3 (20°-35°) is an open angle in which at least the scleral spur can be identified. It is incapable of closure.
Methods of examinationGrading of anglestructures Grade 2 (20°) is moderately narrow angle in which only the trabeculum can be identified. Angle closure is possible but unlikely.
Methods of examinationGrading of anglestructures Grade 1 (10°) is a very narrow angle in which only Schwalbe’s line and the top of the trabeculum can be identified. The risk of angle closure is high.
Methods of examinationGrading of anglestructures Grade 0 (0°) is a closed angle resulting from iridocorneal contact. Indentation gonioscopy with the Zeiss goniolens is neceserry do differentiate between „appositional” and „synechial” angle closure.
Methods of examinationOphthalmoscopy of the opticnervehead The key to the interpretation of visual field loss in relation to optic nerve cupping in glaucoma is an understanding of the distribution of the 1,2 million axons. Fibres arising from the macula an from the nasal retina follow a straight course to the optic nerve head. Those from macula form a spindle-shape area (papillomacular bunge).
Methods of examinationOphthalmoscopy of the opticnervehead Fibres arising from the retina temporal to the macula follow an arcuate path around the papillomacular bundle to reach the optic nerve head.
Methods of examinationOphthalmoscopy of the opticnervehead The arcuate fibres reaching the superotemporal and inferotemporal parts of the optic nerve head are most vulnerable to damage in glaucoma and the fibres of the papillomacular bundle are the most resistant.
Methods of examinationOphthalmoscopy of the opticnervehead The scleral canal is an opening through which nerve fibres leave the eye. The diameter of this canal is related to the size of the optic disc – eyes with small canals have small optic discs (hypermetropia), with large canals – large discs (myopia).
Methods of examinationOphthalmoscopy of the opticnervehead The optic cup is a pale depression in the centre of the optic nerve head which is not occupied by neural disc tissue. Cupping is best evaluated by observing the bending of the small blood vessels as they cross the disc.
Methods of examinationOphthalmoscopy of the opticnervehead The size of the cup is related to the diameter of the disc – a small disc have a small cup because the nerve fibres are bunched and crowded up as they leave the eye.
Methods of examinationOphthalmoscopy of the opticnervehead In adult glaucoma, pathological cupping is caused by a decrease in the number of nerve fibres, glial cells and blood vessels. In young children, cupping may be caused by an increase in the diameter of scleral canal and be reversible with early treatment.
Methods of examinationOphthalmoscopy of the opticnervehead The neuroretinal rim is a tissue between the outer edge of the cup and the outer margin of the disc. A normal rim should be orange or pink and constant, irrespective of the overall diameter of the disc.
Methods of examinationOphthalmoscopy of the opticnervehead The normal c/d ratio in the horizontal meridian in most eyes is 0,3 or less. Only 2% of normals have a ratio of more than 0,7. In 70% of patients with early glaucoma the difference between two eyes is more than 0,1.
Methods of examinationOphthalmoscopy of the opticnervehead The spectrum of disc damage in glaucoma ranges from highly localized tissue loss with notching of the neuroretinal rim to diffuse concentric enlargement of the cup. Concentric expansion of the optic cup is caused by a diffuse loss of nerve fibres. When this occurs the excavation simply enlarges concentrically without associated localized notching of neuroretinal rim.
Methods of examinationOphthalmoscopy of the opticnervehead Localized expansion of the optic cup is caused by localized damage to the neuroretinal rim at the superior or – more commonly – inferior poles of the optic disc.