Download
1 / 24
250 likes | 636 Vues
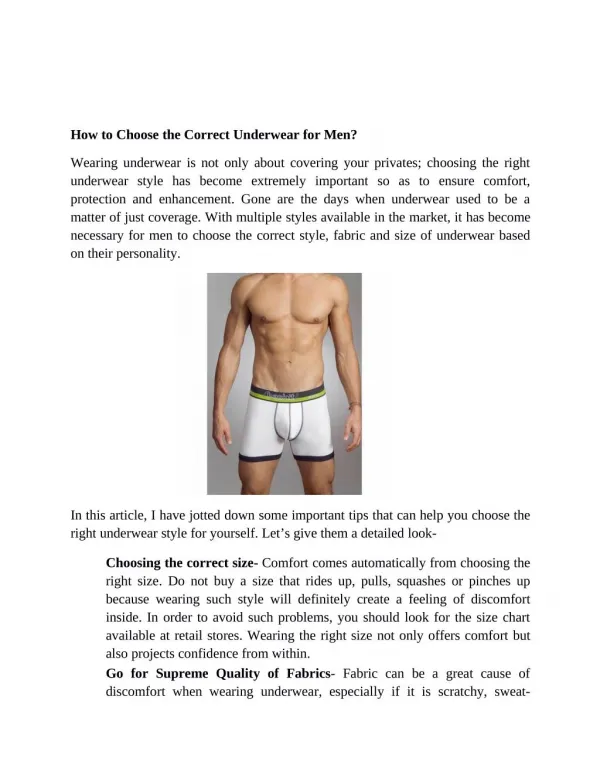
Oesophagectomy: Choosing The Correct Approach. Seamus McHugh. Patient 1. 64 year old male Presented with 7 month history dysphagia and weight loss. OGD + biopsy revealed invasive adenoca of OGJ Pre-op TTE: Severe aortic stenosis, gradient of 70mmHg EF 55% Carotid Duplex:

E N D
Oesophagectomy: Choosing The Correct Approach Seamus McHugh
Patient 1 • 64 year old male • Presented with 7 month history dysphagia and weight loss. • OGD + biopsy revealed invasive adenoca of OGJ • Pre-op TTE: • Severe aortic stenosis, gradient of 70mmHg • EF 55% • Carotid Duplex: • RICA 100% Occlusion • LICA 50-70% Occulsion
Patient 1 • EUS, CT/PET and staging laparoscopy : • cT3N0 lesion at OGJ • No evidence of distant disease • Underwent neoadjuvant radiotherapy and chemotherapy (Cis/5-FU and 40Gy) • Surgery: Transhiatal Oesophagectomy • Currently well on Hardwick ward • Epidural / Urinary catheter removed day 3 • Central line removed day 4 • Niopam swallow day 5
Patient 2 • 50 year old male, presented with dysphagia • OGD and biopsy revealed adenocarcinoma of OGJ • B/G HTN • Underwent 2 cycles of neoadjuvant chemotherapy • Electively admitted for Oesophagectomy
Patient 2 • Underwent 2 stage transthoracic (Ivor Lewis) oesophagectomy 9th Sept • Mobilisation of stomach via upper midline laparotomy • Right posterolateral thoracotomy • Oesphagus mobilised up to azygos • Subcarinal lymph nodes excised • Oesophagus trasected and excised • Tubularised stomach anastamosed at level of T6 • Histology: Adenocarcinoma T3N1Mx. 4/16 lymph nodes positive for malignancy • Discharged day 11 post op
Transhiatal Oesophagectomy (THO) • Originally described by Dent in 1913 • First performed by Turner in 1933 • Subsequently popularized by Orringer[1,2] • Pommier RF, Vetto JT, Ferris BL, et al. Relationships between operative approaches and outcomes in esophageal cancer. Am J Surg 1998; 175:422– 425. • Orringer MB, Marshall B, Iannettoni MD. Transhiatal esophagectomy: clinical experience and refinements. Ann Surg 1999; 230:392– 403.
Ivor Lewis Oesophagectomy (ILO) • Combined abdominal and thoracic approach originally described by Ivor Lewis in 1946 [1] • Lewis I. The surgical treatment of carcinoma of the esophagus, with special reference to a new operation for growths of the middle third. Br J Surg 1946; 34:18 –31.
THO vs ILO • It is argued that the transhiatal operation is less of a physiologic insult on the body. • Conversely, it is argued that THO violates basic surgical principles of adequate exposure and hemostasis, and that lymph node clearance is not as complete with THO as with ILO • Compare THO and ILO in terms of • Morbidity • 5 year survival • Disease free interval
Morbidity • Anastamotic leak older studies… • Leak rates greater than 25% have previously been reported for THO, more than double that which is expected for ILO [1] • The consequences of a leak in the neck are far less disastrous than those with intrathoracic leaks, where mortality after a leak approaches 50% [2] • Vigneswaran, W.T., Trastek, V.F., Pairolero, P.C., Deschamps, C., Daly, R.C., Allen, M.S.: Transhiatal esophagectomy for carcinoma of the esophagus. Ann. Thorac. Surg. 56:838, 1993 • Goldminc, M., Maddern, G., Le Prise, E., Meunier, B., Campion, J., Launois, B.: Oesophagectomy by a transhiatal approach or thoracotomy a prospective randomised trial. Br. J. Surg. 80:367, 1993
Anastamotic leak continued… • Connors et al [1] • 17,395 patients (Nationwide Inpatient Sampling Database) • No difference in GI complications (including anastamotic complications) • Chang et al [2] • 225 THO vs 643 Transthoracic • Anastamotic complication rate higher in THO (43.1% vs 34.5%) but overall mortality similar between both groups • Contemporary studies demonstrated mortality for intrathoracic leaks comparable to cervical [3,4] • Connors RC et al. Comparing outcomes after transthoracic and transhiatal oesophagectomy: A 5-year propective cohort of 17,395 patients. J am Coll Surg.207;205(6):735-740 • Chang AC et al. Outcomes after transhiatal and transthoracic esophagectomy for cancer. Ann Thor Surg. 2008;85(2):424-429 • Briel JW et al. Prevalence and risk factors for ischaemia versus colon interposition. J Am Coll Surg.2004;198(4):536-41 • Martin LW et al. Management of intrathoracic leaks following esophahgectomy. Adv Surg.2006;40:173-90
Gluch et al. Comparison of Outcomes following Transhiatal or Ivor Lewis Esophagectomy for Esophageal Carcinoma. World J. Surg. 23, 271–276, 1999
Hulscher JB, van Sandick JW, de Boer AG, et al. Extended transthoracicresection compared with limited transhiatal resection foradenocarcinoma of the esophagus. N Engl J Med 2002;347:1662–9. • 220 patients with mid/distal adenocarcinoma • 106 THO • 114 TTO • Higher peri-operative morbidity after trans thoracic oesophagectomy • Pulmonary complication rate of 57% vs 27% (THO) • No difference in in-hospital mortality
SCC Distal third of oesophagus n=39 No statistical difference SCC Distal third of oesophagus n=38 No statistical difference Chu KM, Law SY, Fok M,Wong J. A prospective randomized comparison of transhiatal and transthoracic resection for lower-third esophageal carcinoma. Am J Surg 1997;174:320–4. Goldminc M, Maddern G, Le Prise E, et al. Oesophagectomy by a transhiatalapproach or thoracotomy: a prospective randomized trial. Br JSurg 1993;80:367–70. 5 year survival
Omloo JM, Lagarde SM, Hulscher JB, et al. Extended transthoracicresection compared withlimited transhiatal resection for adenocarcinomaof the mid/distal esophagus: five-yearsurvival of a randomizedclinical trial.Ann Surg 2007;246:992–1001. 95 patients underwent THO and 110 patients underwenttransthoracic oesophagectomy. After transhiatal andtransthoracic resection five-year survival was 34% and36% respectively In a subgroup analysis, no overallsurvival benefit for either surgical approach was seen in115 patients with a type II (tumour of the cardia) However, in 90 patients with a type I tumour (distal oesophagus) an absolute survival benefit of 14% was seen withthe transthoracic approach (51% vs. 37%, p0.33).
Rizzetto C, DeMeester SR et al. En bloc esophagectomy reduces local recurrence and improves survival compared with transhiatal resection after neoadjuvant therapy for esophageal adenocarcinoma.J Thorac Cardiovasc Surg. 2008 Jun;135(6):1228-36 • 58 patients between 1992 – 2005 • Neoadjuvant Tx followed by surgery • “En Bloc” resection vs THO • 5 yr survival 51% vs 22% • Concluded that “en bloc” resection afforded a survival advantage in post neo-adjuvant patients
No lymph nodes involved >8 lymph nodes 1-8 lymph nodes 5 year disease free survival Dependant on number of positive lymph nodes in resection [1]: Comparable locoregional disease free survival Locoregional disease free-survival advantage ifoperated via the transthoracic route (23% vs. 64%,p 0.02) • Omloo JM, Lagarde SM, Hulscher JB, et al. Extended transthoracicresection compared withlimited transhiatal resection for adenocarcinomaof the mid/distal esophagus: five-yearsurvival of a randomizedclinical trial. Ann Surg 2007;246:992–1001.
Peyre CG, Hagen JA, DeMeester SR et al. Predicting systemic disease in patients with esophageal cancer after esophagectomy: a multinational study on the significance of the number of involved lymph nodes.Ann Surg 2008 Dec;248(6):979-85 • Multinational retrospective review • 700 Adenoca, 353 SCC undergoing oesophagectomy alone • Systemic disease recurrance: • 40% Overall • 16% if 0 Lymph nodes involved • 93% with >8 involved
The future…? • Minimally invasive procedures increasingly adopted • UK study of 75 oesophagectomies comparing convention and minimally invasive ILO [1] • Laparoscopic appraoch associated with: • Reduced blood transfusion • Decreased operative time • Adequate lymph node harvest • Hamouda AH et al. Perioperative outcomes after transition from conventional to minimally invasive Ivor-Lewis esophagectomy in a specialized center. Surg Endosc 2009 Sep 3 [Epub ahead of print]
Conclusions • In the short term, THO is is accompanied by less morbidity • In the long term, THO seems preferable onlyfor patients with: • Tumours located at the GOJ • Without suspected nodes in the upper compartmentof the chest • Post neoadjuvant patients or poor clinical condition • Transthoracic oesophagectomy: • Tumours located elsewhere in the oesophagus • Junctional tumours with suspectedlymph nodes high in the chest.