Download
1 / 83
840 likes | 1.1k Vues
Tick Borne Illness in Virginia. Thomas M. Kerkering, M.D. Professor of Medicine & Professor Virginia Tech Program of Public Health Chief, Section of Infectious Diseases VTCSOM & Carilion Clinic. 71 year old WM presents with three day hx “heavy chest

E N D
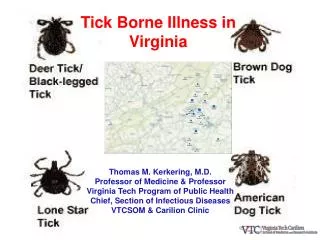
Tick Borne Illness in Virginia Thomas M. Kerkering, M.D. Professor of Medicine & Professor Virginia Tech Program of Public Health Chief, Section of Infectious Diseases VTCSOM & Carilion Clinic
71 year old WM presents with three day hx “heavy chest sensation”, fever, chills, fatigue, dull headache & dyspnea. B/P 199/70, P =102, T = 102.3, R = 20. EKG, troponins not indicative of cardiac ischemia. Tick bites “all the time”; last one 7 days ago. Lyme screening antibody = 3.47 (normal < 0.9) What is your Diagnosis?
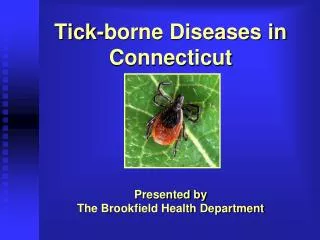
Deer tick, black legged tick, Ixodes scapularis (ehrlichiosis, Lyme disease, babesiosis)
Male & Female Black Legged Tick Deer tick, Ixodes scapularis (ehrlichiosis, Lyme disease, babesiosis)
Male & Female American Dog Tick, (Dermacentor variabilis) Rocky Mountain Spotted Fever
Male & Female Lone Star Tick, (Amblyomma americanum) Ehrilichia chaffeensis, STARI
Anaplasmosis is caused by the bacterium Anaplasma phagocytophilum. This organism used to be known by other names, including Ehrlichia equi and Ehrlichia phagocytophilum, and the disease caused by this organism has been previously described as human granulocytic ehrlichiosis (HGE).
The areas from which cases are reported correspond with the known geographic distribution of the lonestar tick (Amblyomma americanum), which is associated with transmission of both E. chaffeensis and E. ewingii.
RMSF The primary tick that transmits R. rickettsii in these states is the American dog tick (DermacentorvariabilisDermacentorandersoni).
Tick Borne Diseases in Virginia • Babesiosis • Ehrlichiosis • Lyme Disease • Rocky Mountain Spotted Fever • STARI • Tick Paralysis • Tularemia
Cases of Ehrlichiosis / Anaplasmosis By Year in Virginia Significance of Trend p = 0.0001 Source: VDH
Cases of Spotted Fever By Year In Virginia Significance of Trend p = 0.01 Source: VDH
Cases of Lyme Disease By Year in Virginia Significance of Trend p = 0.0002 Source: VDH
Cases of Tularemia By Year in Virginia Significance of Trend p = 0.5 Source: VDH
Babesiosis B. microti on peripheral smear
Babesiosis • incubation period of 1 to 4 weeks • the disease can last several weeks. • more severe in patients who are immunosuppresed, • splenectomized, and/or elderly • infections caused by B. divergens tend to be more • severe (frequently fatal if not appropriately treated) • than those due to B. microti, where clinical recovery • usually occurs.
Clinical Features of Babesiosis • Most infections are probably asymptomatic • Manifestations of disease include • Fever • Chills • Sweating • Myalgias • Fatigue • Hepatosplenomegaly • Hemolytic anemia
Diagnosis of Babesia infection • Made by detection of parasites in patients' blood smears. • Antibody detection tests are useful for: • detecting infected individuals with very low levels of parasitemia (such as asymptomatic blood donors in transfusion-associated cases), • for diagnosis after infection is cleared by therapy, and for discrimination between Plasmodium falciparum and Babesia infection in patients whose blood smear examinations are inconclusive and whose travel histories cannot exclude either parasite. • The indirect fluorescent antibody test (IFA) 88-96% of patients with B. microti infection. Patients' titers generally rise to >1:1024 during the first weeks of illness and decline gradually over 6 months to titers of 1:16 to 1:256 but may remain detectable at low levels for a year or more.
PCR Testing for the presence of B. microti DNA is available.
Ehrlichia chaffeensis primarily infects mononuclear leukocytes (predominantly monocytes and macrophages), The pathogen that causes human granulocytic ehrlichiosis (HGE) (Anaplasmosis)primarily infects granulocytes (neutrophils and rarely eosinophils).
Ehrlichia ewingii primarily infects neutrophils and occasionally eosinophils and produces a disease clinically similar to HME and HGE. Most patients with this form of ehrlichiosis have also had other medical conditions causing immunosuppression (e.g., HIV infection, splenectomy, transplantation,
Lone star tick (Amblyomma americanum) Ehrlichia chaffeensis is principally transmitted by the lone star tick (Amblyomma americanum) White-tailed deer are a major host of lone star ticks and appear to represent one natural reservoir for E. chaffeensis.
Blacklegged tick(Ixodes scapularis) The HGE agent (Anaplasmosis) has been associated with the blacklegged tick (Ixodes scapularis). Deer, elk, and wild rodents are likely reservoirs.
Ehrlichiosis • incubation period of about 5-10 days after the tick bite • Patients with ehrlichiosis generally visit a physician • in their first week of illness • Initial symptoms generally include • - fever • - headache • - malaise • - myalgias
Ehrlichiosis • Other signs and symptoms may include • - nausea • - vomiting • - diarrhea • - cough • - joint pains • - confusion • - occasionally rash. • In contrast to Rocky Mountain spotted fever, rash is relatively uncommon in adult patients with HME, and is rarely reported with HGE. However, rash has been described in approximately 60% of pediatric patients infected with E. chaffeensis.
Ehrlichiosis Laboratory findings indicative of ehrlichiosis include - leukopenia - thrombocytopenia - elevated liver enzymes If a lumbar puncture is performed the CSF is abnormal - a few to 100-200 WBC (predominately lymphs) - a few RBCs - normal glucose - normal to slightly elevated protein
Ehrlichiosis Ehrlichiosis can be a severe illness, especially if untreated, and as many as half of all patients require hospitalization. Severe manifestations of the disease may include: - prolonged fever - renal failure - disseminated intravascular coagulopathy - meningoencephalitis - adult respiratory distress syndrome - - seizures, or coma It is estimated that 2%-3% of patients may die from the infection. Preliminary evidence suggests that E. chaffeensis infection may become more severe than other Ehrlichia infections.
Ehrlichiosis The severity of ehrlichiosis may be related in part to the immune status of the patient. Persons with compromised immunity caused by immunosuppressive therapies e.g., - corticosteroids - cancer chemotherapy - HIV infection - splenectomy appear to develop more severe disease, and case-fatality ratios for these individuals are characteristically higher than case-fatality ratios reported for the general population.
Ehrlichiosis The organisms can be demonstrated in blood smears by staining with Diff-Quik or Giemsa stains
Ehrlichiosis Although IFA remains the principal diagnostic tool for the detection of ehrlichial infection, there is no standardized antigen, conjugate, or agreement on what constitutes a positive result among the various laboratories providing these tests Most patients demonstrate increased IgM or IgG titers by the second week of the illness. However, patients may lack diagnostic IgG antibody titers in the first 7 days of illness. This is an important consideration, because patients seek health care at a median of 3 days after onset of the illness.
Ehrlichiosis PCR is the next most frequently used method for detecting infection. This test is available through CDC and some state health laboratories, as well as a number of research and commercial laboratories. PCR tests remain unstandardized, and analytical and diagnostic sensitivity and specificity may vary among individual assays. Direct isolation of the organism remains the gold standard for confirmatory diagnosis, but is the most difficult and time-consuming approach. Both E. chaffeensis and the HGE agent have been recovered from the blood of acutely ill patients by using a variety of cell lines.
Ehrlichiosis Doxycycline 100 mg twice daily for adults 4.4 mg/kg body weight per day in two divided doses for children under 45.4 kgs (100 lbs) treat for at least 3 days after the fever subsides and until evidence of clinical improvement, for a minimum total course of 5 to 7 days severe or complicated disease may require longer treatment courses. rifampin has been used successfully in a limited number of pregnant women with documented HGE.