Download
1 / 67
680 likes | 931 Vues
Analgesic Ladder in TBI Pain Management. Jim Plunkett, M.D. VA Medical Center/UC Dept of PM&R 2013 NKY TBI Conference March 22, 2013. Chronic Pain. IASP definition “an unpleasant sensory or emotional response to a stimulus associated with actual or potential tissue damage”

E N D
Analgesic Ladder in TBI Pain Management Jim Plunkett, M.D. VA Medical Center/UC Dept of PM&R 2013 NKY TBI Conference March 22, 2013
Chronic Pain • IASP definition • “an unpleasant sensory or emotional response to a stimulus associated with actual or potential tissue damage” • Pain “lasting longer than the anticipated course of recovery” – often 3-6 months • Neurologic, physiologic, and emotional components ( suffering)
Nociceptive Pain • Noxious stimuli activating peripheral receptors producing typical acute pain along a-delta and C fibers • Pin-prick or stab wound or stubbed toe • Burn injury • Fractures
Neuropathic Pain • Pain associated with injury or disease of peripheral nerves • DM peripheral neuropathy • Shingles ( PHN) • Radiculopathy • Burning, shooting, lancinating pain • Allodynia, hyperpathia, central sensitization
Pathology: • Muscle atrophy, • weakness; • Bone loss; • Immunocomprimise • -Depression / Suicide Beginning to End: The Chronic Pain Cycle • Pathophysiology of Maintenance: • Radiculopathy • Neuroma traction • Myofascial sensitization • Brain, SC pathology (atrophy, reorganization) • Psychopathology • of maintenance: • Encoded anxiety • dysregulation • - PTSD • -Emotional • allodynia • -Mood disorder Acute injury and pain • Central • Sensitization • Neuroplastic • changes Disability Less active Kinesophobia Decreased motivation Increased isolation Role loss Peripheral Sensitization: New Na+ channels cause lower threshold Neurogenic Inflammation: - Glial activation - Pro-inflammatory cytokines - blood-nerve barrier dysruption Gallagher RM, in Ebert & Kerns, 2010)
Prevalence of Chronic Pain, PTSD and TBI in a sample of 340 OEF/OIF veterans Chronic Pain N=277 81.5% PTSD N=232 68.2% 16.5% 2.9% 10.3% 42.1% 12.6% 6.8% TBI N=227 66.8% 5.3% Lew, Otis, Tun et al., (in Press). Prevalence of Chronic Pain, Posttraumatic Stress Disorder and Post-concussive Symptoms in OEF/OIF Veterans: The Polytrauma Clinical Triad. JRRD
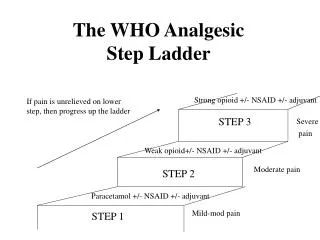
WHO Analgesic Ladder 1986 • Step 1: Non-opioids (tylenol +/- NSAID) • +/- adjuvants • Step 2: “Weak opioids” • + non-opioids +/- adjuvants • Step 3: “ Strong opioids” • + non-opioids +/- adjuvants
Expanded Analgesic Ladder • Activity modification • Thermal modalities • Electrical topical modalities • Topical medical analgesics • Gait and mobility aides • Bracing • Stretching/ROM/massage • Strengthening • Aerobic reconditioning • Basic self-care health habits
Ladder ( con’t) • Non-opioids • Acetaminophen • Aspirin • NSAIDS
Adjuvants • Muscle relaxants • Anti-epileptic drugs ( AEDs) • Anti-depressants • Corticosteroids
Narcotics • Pseudo-narcotics ( tramadol) • Weak potency vs. Strong potency • Short-acting vs. Long- acting • Oral vs. topical vs. transmucosal vs. IV • Combination
Invasive procedures • Basic • Myofascial trigger point injections • Intra-articular injections • Botox – headache and spasticity • Acupuncture • Nerve blocks
Invasive procedures • Advanced: ( Fluoro-guided) • Cervical, thoracic, and lumbosacral ESI • Facet injections • Medial branch blocks • Sacro-iliac joint injections • RF nerve ablation • IDET • Stellate ganglion and LS sympathetic blocks • Celiac plexus block, Bier block
Quaternary Interventions • Spinal Cord ( or Dorsal column) stimulator • Intrathecal Pain pump • Rhizotomy or myelotomy • Deep Brain stimulation • Thalatomy
Cognitive/Behavioral therapies • Progressive relaxation • Guided imagery • Individual and Group therapy • Cognitive/behavioral therapy • Biofeedback
Pain Categories • “Orthopedic” • OA/DJD • Muscles, tendons, ligaments • “Neuropathic” • Myelopathy, radiculopathy • Peripheral neuropathy • Complex/Central Pain
Categories • Above + Chronicity help guide treatment • Other factors – Secondary Gain • Workmen’s Comp, Tort claim, SSDI • Medical co-morbidities • Traumatic Brain Injury • Age
Headache • Episodic Headache • Characterize type • Abortive therapy • Maximum 6 doses/week • Chronic Daily Headache • > 15 HA days per month • Analgesic rebound • Prophylaxis is key Avoid narcotics & Benzos Prophylaxis Onset of action ~ 4 wks Abortive • NSAIDs • GI side effects • Ibuprofen • Naproxen Sodium • Aspirin • Triptans • Contraindicated in • patients with CAD • Combination • Medications • Cognitive side effects • Risk of W/D • Fioricet • Fiorinal • Midrin Alternatives Promethazine Metoclopramide Prochloroperazine Tizanidine Non-medication Trigger point injection Occipital nerve block Physical therapy • Anti-depressants • May improve mood • Improves sleep • Nortriptylline • Amitryptilline • Paroxetine • Fluoxetine • AEDS • Neuropathic pain • gabapentin • Mood lability • valproic acid • topirimate • Beta-blockers • Non-selective may • have benefit on • autonomic effects of • PTSD • Propranolol
Back to Ladder details • Activity modifications • “RICE” + Lifting and positional limitations • Work hours and work pacing • Rotation of repetitive tasks • Ergonomic adjustments • Biomechanical optimization • Graduated return to work
Topical modalities • Ice • Heat • Topical analgesics • Capsaicin • Lidoderm • Camphor, menthol and salicylates ( Ben-gay) • Ultrasound or Iontophoresis ( steroids/NSAIDs) • TENS unit • E-stim, Biovest, Alpha stim • Cold laser
Gait and mobility aides • Cane • Walker incl. Rolling walker w/ fold-down seat • Wheelchair ( manual vs. electric) • Scooter
Orthotics • Lumbar support • Wrist splint +/- thumb spica • Elbow pads, arm sling • Soft cervical collar • Knee brace – hinged/unhinged • Ankle brace or AFO • PTB AFO • Shoe orthotic inserts, sole modifications
PT + HEP • Stretching/ROM/soft tissue mobilization • Strengthening – Isometric -> Isotonic • Work or activity - specific training • Plyometrics • Basic or modified aerobic reconditioning • Walking/treadmill - graduated • Bike riding – upright/recumbent • Aquatic – based • Cardiopulmonary parameters
Massage Therapy • Craniosacral techniques for TBI
Chiropractic • Manipulation • Modalities
Basic Selfcare – Health habits • Obesity – diet • Smoking • Alcohol • Drug abuse • Sleep hygiene • Stress management
Basic analgesics • Acetaminophen ( NTE 4000 mg/day) • Hepatic caveats • ASA • GI monitoring
NSAIDs • Salicylates • Non-acetylated ( Salsalate, Disalcid, Trilisate) • Propionic acids • Ibuprofen, Naproxen, ketoprofen, Oxaprasin • Acetic acids • Indomethacin, diclofenac, sulindac, toradol • Oxicams • Piroxicam • Cox-2 Inhibitors • Celebrex • Xyflamend – herbal - OTC
Muscle relaxants • Cyclobenzaprine ( TCA) • Parafon forte, methocarbamol, carisoprodol • Dantrium • Baclofen • Tizandine • Diazepam • Caveat re sedation and liver function • Soma – ( and valium) dependency
Neuropathic agents • Antidepressants • TCA – ami/nortriptyline, trazodone, desipramine • SSRI’s: • SNRI’s: venlafaxine, duloxetine
Neuropathic agents • Anti-epileptic drugs: • Carbamazepine, oxcarbazepine • Topiramate, Keppra • Gabapentin ( Neurontin) • Pregabalin ( Lyrica) • Watch for CNS SE, drug interactions esp tegretol • LFT and WBC monitoring
Oral steroids • Medrol dospak ( Methylprednisolone) • Prednisone taper ( 40 mg -> 0 over 12 d) • GI, DM, cataract, osteoporosis • But also watch out for Bipolar d/o
Narcotics • Pseudo-narcotic • Tramadol – mu agonist activity • Mild analgesia • Watch for serotonin syndrome w/ SSRI’s • Habit-forming
Narcotics • Mild • Propoxyphene ( Darvocet/Darvon) • No efficacy > tylenol – removed from market • Codeine • Poor GI tolerance • 2-10 % transformation to morphine
Narcotics • Short-acting • Oxycodone – schedule II • Hydrocodone – schedule III-> II • Meperidine ( Demerol) • Hydromorphone ( Dilaudid) • Avoid for chronic pain – rapid accommodation • Morphine IR
Narcotics • Long-acting • OxyContin • Morphine SR, MS Contin • Avinza, Opana • Methadone • Fentanyl patch or lollipop • Tapentadol (Nucynta)
Narcotic SE • Common • N/V • Constipation – proactive bowel regimen • Sedation *** Key to avoid in TBI** • Itching • Physiologic/psychological dependence • Sweating • Anorexia • Myoclonus
Narcotic SE • Myoclonus • Dizziness/orthostasis • Accommodation • Respiratory suppression • Cardiac dysrhythmia – methadone • Methadone also difficult to achieve equianalgesic dosing + occ idiosyncratic buildup w/ long ½ life > analgesic effect
Narcotic Issues • Avoid as unimodal pharmacologic approach – opioid sparing concept • Possible opioid hyperalgesia • May need to rotate type of narcotic if accommodated • Addiction vs Pseudo-addiction ( UDS) • Dependency – physiologic/psychologic • Taper ( 50 %/week) vs. Detox • Buprenex vs. methadone maintenance
PTSD Pain Re-experiencing Avoidance Social withdrawal Memory gaps Apathy Medication effects Pain Altered Arousal Sensitive to noise Concentration Insomnia Irritability Difficulty with decisions Mental slowness Concentration Headaches Dizzy Appetite changes Fatigue Sadness Suicidality Mild TBI Residua Substance Use (Poly) Depression
Conservative management of pain after TBI Rachel Heberling, MD Cincinnati VA Medical Center University of Cincinnati
Why Conservative Pain Management in TBI? • Increased sensitivity to medications • Increased difficulty managing medications, especially prn’s • Increased self-efficacy via self-management • Potentially decreased number of office visits • Cost-effective
Heat • Superficial heat: heating pad, hot shower, hot bath • Deep heat: ultrasound • Effective for pain relief, increased muscle flexibility • Not much evidence, but obviously effective briefly
Cold • Superficial: Ice packs • Deep: cold laser • Cold effective for pain relief and reducing inflammation, but contracts muscles • Unclear mechanism and efficacy of cold laser
STRETCHING! • Muscle has viscoelastic properties • Slow, deep stretch paired with deep breathing necessary • Muscle properties change for ~10 hrs after deep stretch • Evidence not compelling, but pain-relief effect of stretching is very obvious clinically
Other types of Exercise • Aerobic exercise – has huge role in decreasing muscle tension and consequent pain. • Strength training – some role in decreasing pain (e.g. core strengthening), but generally minimized until pain beginning to improve.
Meditation • Increasing base of evidence for the pain relief effects of meditation • Decreases stress • Improved emotional acceptance of pain