Download
1 / 43
430 likes | 472 Vues
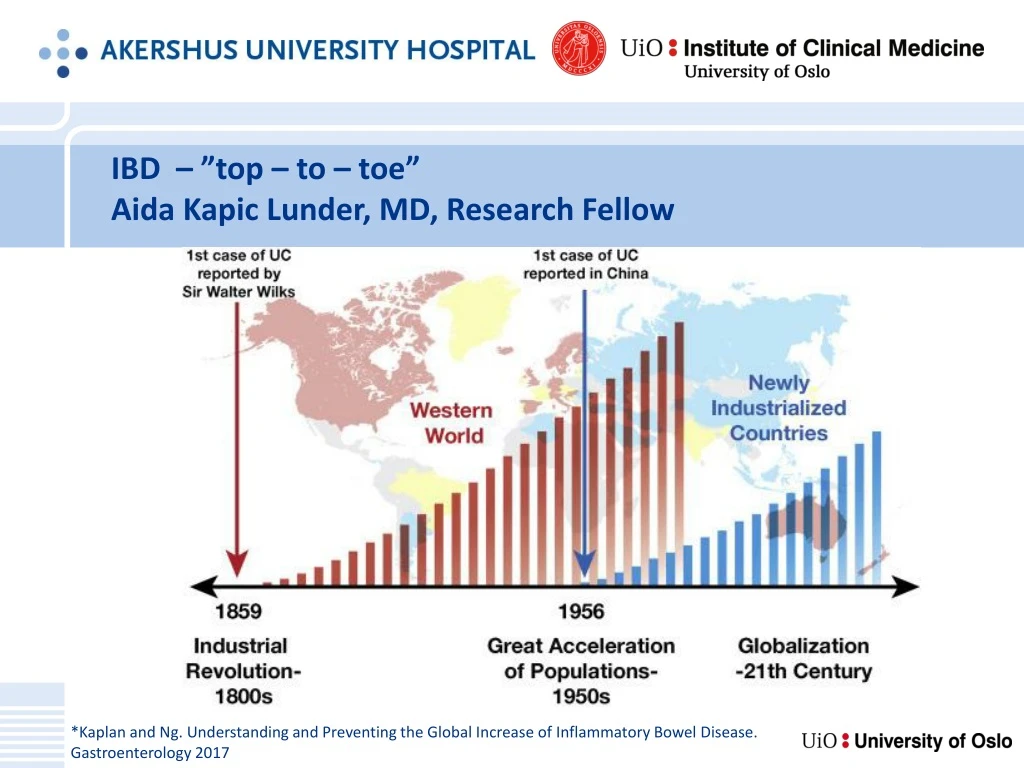
IBD – ” top – to – toe ” Aida Kapic Lunder, MD, Research Fellow. *Kaplan and Ng. Understanding and Preventing the Global Increase of Inflammatory Bowel Disease. Gastroenterology 2017. “ IBD as a systemic disease with a predilection for the gut. ”. Adapted from Baumgart and Sandborn.

E N D
IBD –”top – to – toe” Aida Kapic Lunder, MD, Research Fellow *Kaplan and Ng. Understanding and Preventing the Global Increase of Inflammatory Bowel Disease. Gastroenterology 2017
“IBD as a systemic disease with a predilection for the gut.” Human touch and empathy – with professional skill Adapted from Baumgart and Sandborn
Prevalence of extra-intestinal manifestations (EIM) (6-38%) More common in patients with CD and women
Extra-intestinal manifestations (EIM) Immune mediated Non immune mediated Osteoporosis Cholelithiasis Nephrolithiasis Anemia Urogenital affection Central nervous system affection Cardiovascular affection Pulmonary affection • Arthropathies • Sclerosing cholangitis • Skin disorders • Eye disorders
IBD-related spondyloarthropathy (“gut-synovial axis”) – Most common! Peripheral (5-20%) Axial Inflammatory back pain Spondyloarthritis (16-46%) Ankylosing spondylitis (1-16%) Imaging important! • Symmetric non-deforming arthritis • Usually self-limiting • Large weight-bearing joints • Non-spesific findings: enthesitis, joint effusion, periarticular osteopenia, dactylitis
Spondyloarthritis – ASAS MRI working group(Assessment in SpondyloArthritis International Society) Active inflammatory lesions Structural damage lesions Subchondral sclerosis Erosions Fat deposition Ankylosis (bone bridging) • Bone marrow edema/osteitis • Synovitis • Enthesitis • Capsulitis Lambert et al. Defining active sacroiliitis on MRI for classification of axial spondyloarthritis: update by the ASAS MRI working group. Annals of the rheumatic diseases. 2016.
CT lesions Prakash D et al. Seronegative spondyloarthropathy-related sacroiliitis: CT, MRI features and differentials. Indian J Radiol Imaging 2014;24:271-8
Sacroiliitis, MR enterography T2 FS • 57 y male, CD and PSC Ossum et al. Ankylosing spondylitis and axial spondyloarthritis in patients with long-term inflammatory bowel disease: Results from 20 years of follow-up in the IBSEN study. Journal of Crohn's & colitis. 2017.
Ankylosing spondylitis (1-16%) • Diagnosed when both the • clinical criteria (back pain, stiffness and/or limitation of motion) and • the imaging criteria for sacroiliitis (grade 2 or more bilaterally or grade 3-4 unilaterally) • are met.
Primary sclerosing cholangitis (PSC) – most severe! • 70-80% PSC patients have IBD • 1.4-7.5% IBD patients have PSC
“A patchwork of different phenotypes” The PSC Institute, Rikshospitalet, Norway
Diagnostic work-up • Tricky diagnostics (symptoms? alkaline phosphatase levels?) • MR cholangiography (sens 80 %, spes 87 %) • ERCP • Biopsy – Small duct PSC 5-10 % • Complications? risk of colorectal cancer (x 5) risk of cholangiocarcinoma (x160-1500) Follow-up!
PSC on MRC Strictures Dilatations Mural irregularities Beading Lunder et al. Prevalence of Sclerosing Cholangitis Detected by Magnetic Resonance Cholangiography in Patients With Long-term Inflammatory Bowel Disease. Gastroenterology. 2016;151(4):660-9.e4.
CCA – 5-15 % life time incidence in patients with PSC! • Overlapping imaging findings • Look for: • Focal thickening • Focal Biliary dilatation • Capsular retractions • Portal vein invasion • Fibrous tissue in CCA delayed enhancement
PSC with hilar cholangiocarcinoma (Klatskin tumor) Hussain S. M. et al (2015). Liver MRI: Correlation with other imaging modalities and histopathology, second edition. Springer International Publishing.
Immune-mediated conditions: Skin • Enterocutaneous fistulas (30%) • Aphthous stomatitis (1-10%) • Erythema nodosum (2-15%) • Pyoderma gangrenosum (0.5–2%)
Immune-mediated conditions: Eye • Uveitis (0.5-3.0%) • Episcleritis (0.2%)
Enterogenital fistulas Olpin et al. Beyond the Bowel: Extraintestinal Manifestations of Inflammatory Bowel Disease, radiographics.rsna.org
Obstructive nephropathy (1.9-6% in CD) Olpin et al. Beyond the Bowel: Extraintestinal Manifestations of Inflammatory Bowel Disease, radiographics.rsna.org
NECT Kidney stones (12% in CD) Brisbane et al. An overview of kidney stone imaging techniques. Nat Rev Urol. 2016 November.
Hepatic steatosis (≈35%) • Due to chronic malnutrition, protein loss, corticosteroid therapy? Lee SS et al . Nonalcoholic fatty liver disease. World J Gastroenterol 2014 June 21; 20(23): 7392-7402
Coagulopathy venous tromboembolism Surgical intervention Exacerbation
Case courtesy of Dr Bruno Di Muzio, Radiopaedia.org, rID: 44167 24-year old male with known CD, abdominal distention and vomiting. Treated with partial right colon and distal ileum resection 1,5 year ago.
Osteoporosis (15%) • Etiology: inflammatory-mediated bone resorption, malabsorption, poor diet, corticosteroids, reduced physical activity • Underdiagnosed... L1- values ≤135 HU: Sens 76%, Spes 75% for osteoporosis
Neurological manifestations • Rare, secondary? Drug-induced?
Multiple sclerosis – remitting relapsing type Treated with ileocoecal resection in 2013 Under immunosuppressive treatment quiescent CD and MS today
Which EIMs are attributable to IBD? To what extent? • 56,097 IBD patients were matched to 280,382 non-IBD controls • Associated with IBD: PSC (OR = 188.25), pyoderma gangrenosum (OR = 29.24), ankylosing spondylitis (OR = 7.07), erythema nodosum (OR = 5.95), uveitis (OR = 2.81), sacroiliitis (OR = 2.79), non-rheumatoid inflammatory arthritides (OR = 2.66)
Aims of diagnostic imaging • Assess and characterize: • Disease extent • Disease activity Establish the diagnosis of IBD • Assess • Complications • Systemic manifestations of IBD • Characterize CD behavior: • Inflammatory • Fibrostenosing • Fistulizing Suggest additional examinations
Summary • IBD is a systemic disease with increasing incidence rates • Radiologic imaging is indispensable in modern care of IBD patients • CT and MR techniques offer excellent imaging of intra- and extra-luminal disease • Get used to reporting complications and other manifestations of IBD! Avoid “Satisfaction of search”!
References • Card TR, Langan SM, Chu TP. Extra-Gastrointestinal Manifestations of Inflammatory Bowel Disease May Be Less Common Than Previously Reported. Digestive diseases and sciences. 2016;61(9):2619-26. • Harbord M, Annese V, Vavricka SR, Allez M, Barreiro-de Acosta M, Boberg KM, et al. The First European Evidence-based Consensus on Extra-intestinal Manifestations in Inflammatory Bowel Disease. Journal of Crohn's & colitis. 2016;10(3):239-54. • Kaplan GG, Ng SC. Understanding and Preventing the Global Increase of Inflammatory Bowel Disease. Gastroenterology. 2017;152(2):313-21.e2. • Baumgart DC, Sandborn WJ. Crohn's disease. Lancet (London, England). 2012;380(9853):1590-605. • Olpin et al. Beyond the Bowel: Extraintestinal Manifestations of Inflammatory Bowel Disease, radiographics.rsna.org • Pickhardt PJ, Pooler BD, Lauder T, del Rio AM, Bruce RJ, Binkley N. Opportunistic Screening for Osteoporosis Using Abdominal Computed Tomography Scans Obtained for Other Indications. Ann Intern Med. 2013;158:588–595. doi: 10.7326/0003-4819-158-8-201304160-00003 • Brisbane et al. An overview of kidney stone imaging techniques. Nat Rev Urol. 2016 November.
References • Ossum AM, Palm O, Lunder AK, Cvancarova M, Banitalebi H, Negard A, et al. Ankylosing spondylitis and axial spondyloarthritis in patients with long-term inflammatory bowel disease: Results from 20 years of follow-up in the IBSEN study. Journal of Crohn's & colitis. 2017. • Lambert RG, Bakker PA, van der Heijde D, Weber U, Rudwaleit M, Hermann KG, et al. Defining active sacroiliitis on MRI for classification of axial spondyloarthritis: update by the ASAS MRI working group. Annals of the rheumatic diseases. 2016. • Radiopaedia • Lunder AK, Hov JR, Borthne A, Gleditsch J, Johannesen G, Tveit K, et al. Prevalence of Sclerosing Cholangitis Detected by Magnetic Resonance Cholangiography in Patients With Long-term Inflammatory Bowel Disease. Gastroenterology. 2016;151(4):660-9.e4. • Hussain, S. M. et al (2015). Liver MRI: Correlation with other imaging modalities and histopathology, second edition. Springer International Publishing. • Prakash D et al. Seronegative spondyloarthropathy-related sacroiliitis: CT, MRI features and differentials. Indian J Radiol Imaging 2014;24:271-8 • Lee SS et al . Nonalcoholic fatty liver disease. World J Gastroenterol 2014 June 21; 20(23): 7392-7402
Thank you! Human touch and empathy – with professional skill
