SHOCK!!
SHOCK!!. Justin Bright, M.D. Emergency Physicians of NW Ohio February 20, 2013. The Plan For Today. Define shock What it means physiologically The different types of shock Discuss treatment modalities Discuss ways we handle shock in our ED Make this fun and interesting


SHOCK!!
E N D
Presentation Transcript
SHOCK!! Justin Bright, M.D. Emergency Physicians of NW Ohio February 20, 2013
The Plan For Today • Define shock • What it means physiologically • The different types of shock • Discuss treatment modalities • Discuss ways we handle shock in our ED • Make this fun and interesting • Reward you with chocolate
What is Shock? • Circulatory insufficiency that creates imbalance between oxygen supply and demand • Global tissue hypoperfusion • Causes metabolic acidosis • Left untreated, progresses to end organ failure
Why Is Shock A Big Deal? • People in shock are the most critically ill patients in our ED • Shock = “actively trying to die” • 30-45% of septic shock patients, and 60-90% of cardiogenic shock patients die within 1 month of presentation • Quick decision making and adequate treatment can prolong life
Pathophysiology • Systemic oxygen delivery is a result of arterial O2 content (CaO2) and cardiac output (CO) • A normal Hgb molecule contains 4 O2 molecules • Tissue takes one O2 (25%), leaving 75% O2 content returning to the heart in venous circulation
Compensation • When there is a supply/demand imbalance, the body attempts to compensate • Pumps out more blood (increased CO) • Extracts more O2 (decreases SVO2) • When compensation fails, the body switches over to anaerobic metabolism • Increases lactate levels in the blood
More Compensation • Arteriolar vasoconstriction to redistribute blood flow • Constriction of venous capacitance vessels to increase VR • Release of catacholamines • Release of ADH and activation of renin-angiotensin system
What’s Happening At The Cellular Level? • ATP gets depleted • Na/K ATPase can no longer function • Pump dysfunction causes cellular edema • Cells become less responsive to stress hormones • Lyosymes get released • Cellular integrity is lost and cells rupture • Hemoconcentration, hyperkalemia, hyponatremia, prerenal azotemia, loss of glycemic control, lactic acidosis
General Management Plan • The ABCDE’s of shock • A: airway management • B: reduce work of breathing • C: insure adequate circulation • D: adequate oxygen delivery • E: achieving endpoints of resuscitation
What Are The Types of Shock? • Septic Shock • Cardiogenic Shock • Hypovolemic Shock • Distributive Shock • Anaphylaxis • Neurogenic shock
What Is Septic Shock? • Sepsis is a systemic inflammatory response to infection • This major inflammatory response leads to • Depression of cardiac activity • Large scale vasodilation • Increased metabolic consumption
Septic Shock • Where are the most common sites of infection? • Chest • Abdomen • Urinary Tract
Constitutional Hyperthermia or hypothermia Tachycardia Wide pulse pressure MS changes tachypnea Cardiovascular Hypotension that does not respond well to fluids Cardiac depression Due to coronary hypoperfusion with resultant cardiac ischemia Clinical Features of Septic Shock
Renal Acute renal failure Pulmonary SS is the most common cause of ARDS Significant, non-cardiogenic pulmonary edema Hematologic Neutropenia, thrombocytopenia, DIC Endocrine Hyperglycemia, even in the non-diabetic Poor glycemic control in critical patients is correlated with a much poorer outcome Clinical Features of Septic Shock
Septic Shock • Back in the olden days • Patients in septic shock would sit in the ER for hours waiting for a bed • They’d get some fluids • Maybe some antibiotics • Then they’d go the ICU and die
Take A Moment…. • …To Bow Down To The ER God
The Gist of EGDT • While the patient is sitting in the ED, you optimize treatment early • There are well defined optimization end points • Patient goes to the ICU…. • ….and they live! • Most of the time
Why EGDT is a Big Deal • It has received the most buzz, and produced the most significant change in EM practice in the 21st century • Clinical data shows it significantly improves patient outcomes • Two of our attendings trained under Dr. Rivers • We are good, but not great at EGDT
What Does EGDT entail? • Filling up the tank • Insuring adequate MAP • Insuring adequate SVO2 • Reducing work of breathing, which reduces metabolic demand • Giving pressure support as needed • Giving antibiotics
EGDT • How do we reduce work of breathing? • Oxygenation by NRB • Very low threshold for intubation
Filling Up The Tank • Septic shock causes major vasodilation • Typically will give fluid bolus with minimal BP response • How do we know we’ve given enough fluids? • Central venous pressures (CVP) • Done off a central line • Goal is between 8-12 mmHg
What About The SVO2 and the MAP? • To increase the SVO2, blood transfusion is often necessary • A goal is SVO2 of 70% • To increase the MAP, pressure support medications are often needed • Goal is a MAP between 65 and 90
Pressors in Septic Shock • Dopamine • Increases heart rate and blood pressure • Levophed (norepinephrine) • Increases blood pressure without affecting HR • Dobutamine • Increases HR without really affecting BP
Antibiotics • Blood cultures obtained before antibiotics if possible • Antibiotics given empirically • Will depend on patient comorbidities and history • Ideally will cover against both gram+ and gram- bacteria
Labs ordered CBC Lytes Blood culture UA Coaggs ABG Lactate Blood type and cross Studies CXR or AAS Procedures Central line A-line Foley Intubation So How Will It All Go Down?
Hypovolemic Shock • Due to deficiency in intravascular volume • 3 different categories • Hemorrhage • Trauma, surgery, GI bleeding • Intravascular volume loss • Gastroenteritis, burns, diabetes insipidus, heat stroke • Interstitial loss • Burns, sepsis, nephrotic syndrome, bowel obstruction, ascities
Treatment of Hypovolemic Shock • ABC’s • Volume expansion • Repetitive bolus and re-assessment • If no hemodynamic improvement after 2-3 boluses, patient should get blood products
Cardiogenic Shock • Decreased cardiac output producing inadequate tissue perfusion despite adequate or excessive circulating volume • Causes • Massive AMI causing LV dysfunction • Depression of cardiac contractility • CHF, sepsis, contusion • Obstruction of forward flow • Stenosis, myxoma, HCOM • Regurgitation of LV output • Valve deficiency
Studies EKG CXR Cardiac echo Labs Chest-O BNP lactate What Will We Order?
Clinical Findings in Cardiogenic Shock • Tachypnea • Cool, mottled extremities • Significant peripheral edema • JVD • Cardiac murmurs
Treatment of Cardiogenic Shock • ABC’s • Central line and a-line • If due to AMI • Heparin, ASA, cath lab
Hypotension in Cardiogenic Shock • Excessive fluid administration is contraindicated • Problem is not volume, its that there’s no means to push the blood around • Very small fluid challenges (250 cc)
Pressure Support in Cardiogenic Shock • Dobutamine and milrinone are your friends • Increase contractility • Can’t use if SBP < 90 because have vasodilatory properties • Dopamine alone is bad news increases cardiac workload too much • Has been shown to work well when used in conjunction with dobutamine
Cardiogenic Shock • What do these patient’s need more than anything • Reperfusion with a quickness • Cath lab is better than thrombolytics • Intraaortic balloon pump helps by decreasing afterload and decreases cardiac work
Distributive Shock • Anaphylaxis • Neurogenic
Anaphylaxis • A severe systemic hypersensitivity reaction • Multisystem involvement • May include airway compromise and significant hypotension • Caused by a massive release of a cascade of inflammatory mediators from mast cells and basophils
Risk Factors for Anaphylaxis • Those with severe asthma or previous history of anaphylaxis are at risk for fatal or near-fatal anaphylactic episodes • Recurrence risks are not 100% • 40-60% for insect stings • 20-40% for radiocontrast • 10-20% for penicillin • Atopic individuals are NOT considered to be at any greater risk
Clinical Features of Anaphylaxis • Diffuse uticaria and angioedema • Nausea/vomiting • Bronchospasm • Conjunctivitis and rhinorrhea • Hypotension • Symptoms tend to occur within 60 minutes of exposure
Anaphylaxis Pathophysiology • Mast cell and basophil degranulation and mediator release • Causes IgE mediated reaction • Complement activation • Process requires a previous exposure
So What Do We Do About It? • ABC’s • Single most important step is administration of epinephrine • Decontamination/removal of offending agent
Epinephrine • Research shows epi is underused in anaphylaxis • Start by giving epi bolus (0.1mg) IV • If refractory, then given epi drip at 1-4 mcg/min • if Sx less severe, can give IM epinephrine
After Epi…. • Fluids for hypotension • Steroids (Solumedrol 125mg IV) • Antihistamines • Benadryl (50mg IV) is a H1 blocker • Pepcid (20mg IV) is a H2 blocker • H2 blockers are controversial, but our attendings tend to use them won’t harm patient, might help • Albuterol + Atrovent nebulizers for bronchospasm
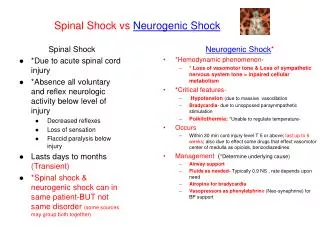
Neurogenic Shock • Occurs after acute spinal cord injury • Causes disruption of sympathetic chain • Leaves unopposed vagal tone (PNS) • Causes hypotension and bradycardia • Neurogenic shock is NOT the same as spinal shock • Spinal shock resolves within 48 hours and is due to swelling around the spinal cord