Download
1 / 31
310 likes | 503 Vues
Common Viral Infections: Influenzaviruses and Herpesviruses. Tintinalli: Chapter 143. Influenza A & B. Antigenic drift Minor mutations of the H or N molecule Antigenicity changes with mutations Causes annual epidemics (usually type A) Antigenic shift

E N D
Common Viral Infections:Influenzaviruses and Herpesviruses Tintinalli: Chapter 143
Influenza A & B • Antigenic drift • Minor mutations of the H or N molecule • Antigenicity changes with mutations • Causes annual epidemics (usually type A) • Antigenic shift • New virus produced by genetic reassortment within a host infected by two different influenzaviruses • Population lacks immunity against new virus • Causes major flu pandemics (such as in 1918)
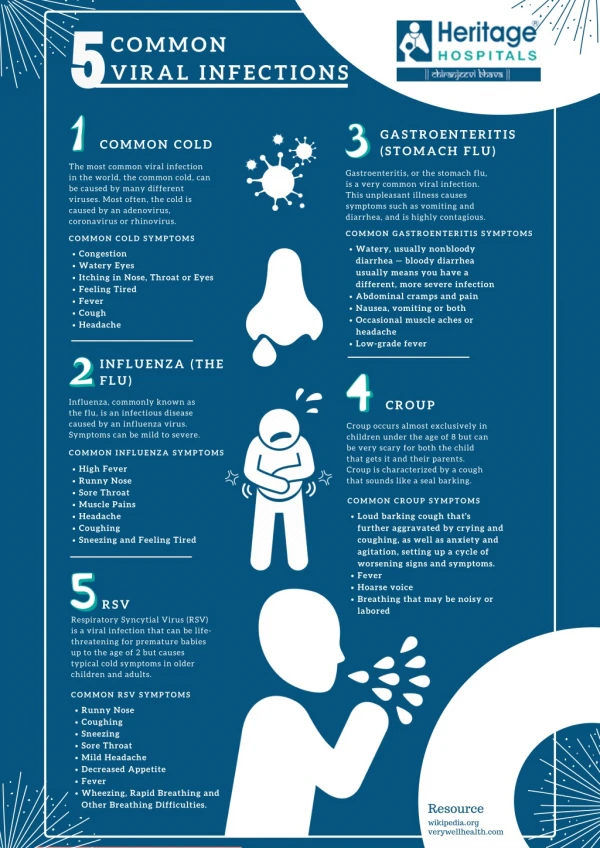
Influenza • Epidemiology • Occurs Nov. thru April in the U.S. • Occurs year-round in the tropics • Spread via droplets produced during cough • Incubation period is 2 days • Viral shedding (contagiousness) starts 24 hours before onset of symptoms • Single-stranded RNA virus (orthomyxovirus)
Influenza • Clinical features (onset is usually rapid) • Fever (38.6o – 39.8o) for 2-4 days • Chills/rigor • Headache • Myalgias/arthralgias • Malaise • Cough • Rhinorrhea • Sore throat with bilat. tender cervical lymphadenopathy • Elderly often do not have classic symptoms and may have only fever, malaise, confusion, and congestion
Influenza • Diagnosis • Clinical diagnosis during outbreak has an accuracy of about 85% • Rapid antigen tests • Decrease empirical antibiotics • Sensitivity 57-81% • Specificity 93-100%
Influenza • Complications • Pneumonitis (high mortality) • Flu symptoms progressing to cough and dyspnea • Hypoxia • Bilateral infiltrates on CXR similar to ARDS • Supportive treatment • Secondary Bacterial Pneumonia • Occurs 1-2 weeks after flu; common in elderly; DM • Treat with broad spectrum antibiotics and pulmonary support • COPD, Reye syndrome (with aspirin use), croup, myocarditis, Guillian-Barre syndrome, pericarditis are also rare complications
Influenza • Treatment • Amantadine and rimantadine (100 mg BID X 5 days) • Approved for type A only; not active against type B • If started within 48 hours of onset of symptoms, it can reduce duration of symptoms by 1-2 days • Avoid both drugs in pregnancy • Approved for children over 1 year of age • Amantadine can cause increase in seizure activity in pts with previous hx of seizure disorder • Oseltamivir and zanamivir (Tamiflu and Relenza) • Active against types A & B • Reduces duration of symptoms by 1 day if started within 48 hours of onset of symptoms
Influenza • Prophylaxis • Annual formulation contains 2 strains of type A and 1 strain of type B • 70-90% effective in those under age 65 • Recommended for all persons over age 65, residents of chronic care facilities, patients with chronic cardiopulmonary disease, diabetes, metabolic disease, or renal disease; immunosuppressed patients, and healthcare workers • Safe for pregnant/lactating women • Anti-influenza medicines are 75-90% effective in preventing influenza if given as a 6-8 week course during peak flu season
Herpesviruses • Enveloped DNA virus • Dwell in host as a lifelong latent infection • May cause clinical disease at a time distant from the primary infection • Some are carcinogenic • Varicella-zoster virus (VZV) is spread via aerosolized particles and close contact • Herpes simplex virus (HSV) and Epstein-Barr virus (EBV) transmission occurs during asymptomatic shedding
Herpes Simplex 1 & 2 • Epidemiology • Transmitted via contact with infected secretions (saliva or genital) on mucous membranes or open skin • HSV-2 is primarily transmitted sexually
Herpes Simplex 1 & 2 • Oral HSV • Primarily HSV-1, but can be HSV-2 • Primary lesion lasts 1-2 weeks • Lesions recur in 60-90% of infected people • Recurrences triggered by local trauma, illness, or stress • Treatment: acyclovir 400 mg PO 5 times/day (topical acyclovir is ineffective) • Prophylaxis: oral acyclovir reduces outbreaks by 50-75% in those with frequent/severe outbreaks
Herpes Simplex 1 & 2 • Genital HSV • Majority caused by HSV-2 • Genital lesions carry small threat to intrauterine infxns in pregnant pts; c-section if active lesions at time of delivery • Ocular HSV • Usually HSV-1 • Ulcerative keratitis is most common manifestation. May lead to corneal blindness • Vesicles may be seen on the conjunctiva or lid • Fluorescein stain may show corneal dendritic ulcers • Ophthalmologic consultation is imperative, and patient may need to be admitted for IV acyclovir
Herpes Simplex 1 & 2 • Encephalitis • Usually HSV-1 • Temporal lobes are the major target and lesions may be seen on CT and MRI • Presents as headache, fever, and altered mental status with preceding viral-like illness. Patients may have olfactory hallucinations • CSF findings: elevated WBCs with mononuclear predominance; dx is PCR of DNA of HSV • Empirical treatment with IV acyclovir at 10 mg/kg every 8 hours should be initiated if suspicion exists • If untreated, mortality rate is 70%
Herpes Simplex 1 & 2 • Bell Palsy • Usually HSV-1 • Causes palsy of the peripheral branch of CN VII • Presents as facial hemiplegia or hemiparesis, taste disturbance, decreased blinking, dry eyes, facial numbness, and jaw/face pain • Central CN VII lesions spare the forehead but cause unilateral lower facial weakness. Peripheral lesions result in forehead paralysis. Attempting to close the eye on the affected side results in an upward gaze (Bell phenomenon)
Herpes Simplex 1 & 2 • Bell Palsy • Examination of the ear, tympanic membrane, mastoid, and parotid gland should be normal • Bell palsy with otitis media, mastoiditis, or parotitis is an ENT emergency • Vesicles on the TM or canal is diagnostic of Ramsay Hunt syndrome • Differential includes stroke, tumor, atypical Guillain-Barre, and Lyme disease • Treatment: prednisone 60 mg PO X 5 days, then tapered for 5 days with acyclovir 400 mg 5 times/day for 10 days • Eye care with artificial tears is the most important therapeutic intervention made by the ED physician
Herpes Simplex 1 & 2 • Herpetic Whitlow • HSV infection of the finger (usually one digit) • HSV-1 is seen in children who self-inoculate during an episode of oral herpes and in health care workers (dentists) • HSV-2 more common if digital/genital contact • Very painful and accompanied by axillary adenopathy • Vesicles contain necrotic epithelial cells, not pus. If confused with paronychia and the finger is incised, delayed healing and secondary infection may occur • Spontaneously heals in 2-3 weeks, may use acyclovir
Herpes Zoster: Chickenpox • HZV is human herpesvirus 3 • Primary infection is chickenpox • Reactivates later as zoster (shingles) • Epidemics occur late winter/early spring • Spread via respiratory droplets • Patients are infectious 48 hours before rash appears until the vesicles have crusted over • Rash appears 14 days after exposure. The virus becomes latent in a dorsal root ganglion
Herpes Zoster: Chickenpox • Clinical features • Prodrome of 1-2 days of fever, malaise • Clear vesicles on an erythematous base appear on the face and trunk, then spread centripetally to the extremities. New lesions will appear and the old ones will become turbid and scab over. The hallmark of chickenpox is vesicular lesions in various stages • Complications can include encephalitis, cerebellar ataxia, pneumonitis, and Reye syndrome • Mortality rate among adults is 15 times higher than in children • Chickenpox during pregnancy can cause fetal abnormalities
Herpes Zoster: Chickenpox • Treatment • Over age 12 • Acyclovir 800 mg PO QID X 5 days (started within 24 hours of onset of rash) • Neonates of mothers who developed chickenpox 5 days before delivery or within 48 hours postpartum • Varicella-zoster immune globulin (VZIG) to confer passive immunity • Patients with varicella encephalitis, pneumonitis, or who are immunocompromised should be admitted for IV acyclovir • Varicella vaccine recommended for children over age 1 year. It is a live vaccine and is contraindicated in immunocompromised patients and in pregnant/lactating women
Herpes Zoster: Shingles • Reactivation of latent VZV infection • Lifetime incidence of 20%, usually in elderly • Lesions limited to a single dermatome, usually thoracic or lumbar • Begins as a prodrome of pain for 1-3 days in the affected area, followed by a maculopapular rash that progresses to vesicles • Disease course is 2-4 weeks • Disseminated disease can cause pneumonitis, hepatitis, or meningoencephalitis
Herpes Zoster: Shingles • Complications: • Herpes zoster ophthalmicus (HZO) • Involves the ophthalmic branch of CN V • Vision-threatening • Hutchinson sign (lesion of tip of nose) may be seen before ocular involvement • May also see a dendriform corneal ulcer with fluorescein staining • Mandatory ophthalmologic consult
Herpes Zoster: Shingles • Complications: • Ramsay Hunt syndrome • Involves the geniculate ganglion of CN VII • Presents with facial palsy, unilateral weakness, loss of taste, and ear canal or TM vesicles • May also see intraoral lesions • May be a cause of mental status change in elderly • Presentation and treatment are similar to Bell palsy • Admit immunocompromised patients for IV acyclovir
Herpes Zoster: Shingles • Complications: • Postherpetic neuralgia • Most common complication • Occurs in 10-20% of all shingles cases, and in 70% of patients over age 70 • Resolves in 1-2 months • First-line treatment is systemic analgesics; second-line treatment is amitriptyline or carbamazepine • Corticosteroids improve quality-of-life in elderly • Start 21-day taper at 60 mg PO daily
Epstein-Barr Virus: Infectious Mononucleosis • Human herpesvirus 4 • Spread by close contact, such as kissing • Incubation period of 1-2 months, followed by prodrome of malaise, fatigue, and fever • Classic symptoms include fever, sore throat (exudative pharyngitis), lymphadenopathy, splenomegaly, and atypical lymphocytosis. Bilateral tender cervical adenopathy is universal • Hepatomegaly and jaundice is common in adults
EBV: Infectious Mononucleosis • Palpable splenomegaly occurs in ½ of patients, most prominent during week 2 of the illness • The incidence of splenic rupture is 0.1-0.5% and is generally at week 2-3 of the illness. Patients should be instructed to avoid contact sports and strenuous activity for 4 weeks • Complications of mono include hemolytic anemia, thrombocytopenia, encephalitis, meningitis, obstructive tonsillitis, and lymphoma
EBV: Infectious Mononucleosis • Lab analysis may show elevated WBC with increased atypical lymphocytes and monocytes • Commercial tests (monospot) are 78-83% sensitive and 98-100% specific. Patients with classic EBV symptoms and a negative monospot should have a repeat monospot in 1 week • Treatment is supportive. If penicillin is given to treat a suspected strep pharyngitis, 95% of patients will develop a rash
Cytomegalovirus • Human herpesvirus 5 • Causes a primary illness and then exists in a latent state in the host until reactivation • Found in milk, saliva, urine, semen, and cervical secretions • Also transmitted during blood transfusions and bone marrow and organ transplantations • One of the TORCH agents known to cause intrauterine infections
Cytomegalovirus • Infection is usually asymptomatic, but symptoms can include fever, chills, myalgias, and headache. Fever may last for 1-5 weeks • May see atypical lymphocytosis, splenomegaly, lymphadenopathy, and increased LFTs • Consider CMV in patients with mono-like symptoms but who are monospot negative
Cytomegalovirus • 10% of AIDS patients develop CMV retinitis, which causes floaters or decreased vision. Fundoscopic exam may show retinal hemorrhages or exudates. Without treatment, this will progress to blindness • Treat with IV ganciclovir or foscarnet
Cytomegalovirus • CMV causes significant morbidity and mortality in post-transplant patients • Pneumonia is the most common infection • Most common in bone marrow transplant patients • CMV should be considered for a fever within 3 months of a transplant
Cytomegalovirus • Treat CMV with ganciclovir or foscarnet • Ganciclovir is approved for CMV retinitis in AIDS patients and for CMV prevention in transplant patients • Foscarnet is used for resistant CMV infections or for patients unable to take ganciclovir • Neither medication cures patients of CMV, but they suppress the acute disease process