Download
1 / 25
450 likes | 1.72k Vues
Vaginal Breech Delivery. Objectives Incidence and Significance Selection Management Intrapartum Delivery. Definition longitudinal lie breech or lower extremity presenting cephalic pole in the uterine fundus Types frank - flexed hips, extended knees

E N D
Objectives • Incidence and Significance • Selection • Management • Intrapartum • Delivery
Definition • longitudinal lie • breech or lower extremity presenting • cephalic pole in the uterine fundus • Types • frank - flexed hips, extended knees • complete - flexed hips, flexed knees • footling - extended hip(s)
Types of Breech Frank Footling Complete
Incidence • 3 to 4% of all pregnancies • increases with decreasing gestational age • 7 to 10% at 32 weeks • 25 to 35% at < 28 weeks
Etiology of Breech Presentation • idiopathic • prematurity (head to trunk size) • uterine or pelvic structural abnormality • uterine fibroid • fetal anomaly or abnormality • polyhydramnios • multiple gestation
Diagnosis • maternal perception of movement • Leopold’s maneuvers • FH auscultated above umbilicus • vaginal exam • ultrasound • X-ray
Recommendations for Breech Delivery • recommend trial of labour at 36 weeks or when estimated weight is 2500 to 4000 grams • offer trial of labour at 31 to 35 weeks gestation or when estimated weight is 1500 to 2500 grams • offer caesasean section at 30 weeks gestation or when estimated weight is < 1500 grams* • no recommendation for when estimated weight is > 4000 grams* * acknowledged lack of evidence for recommendation
Selection Criteria for Trial of Labour • frank or complete breech • fetal head not hyperextended • estimated fetal weight 2500 to 4000g
Ultrasound Assessment • confirm lie and type of breech • assess head position • obtain estimate of fetal weight • assess for IUGR and congenital anomalies • assess amniotic fluid volume • confirm placental localization
Contraindications to Trial of Labour • fetal or maternal contraindication to labour • footling breech • hyperextension of the fetal head • absence of informed consent • absence of experienced maternity health care giver
Management in Labour • planned delivery in hospital • admission in early labour or with ROM • appropriate fetal surveillance • epidural and ARM for usual indications • immediate vaginal exam at ROM to rule out cord prolapse • good progress in labour ( 0.5 cm/h after 3 cm) • induction and augmentation permissible
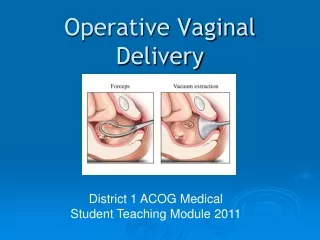
Management at Delivery • experienced newborn resuscitator present • empty maternal bladder • maternity attendant with experience in breech delivery • forceps if available, may be helpful
Entering the Pelvis Obstetrics - Normal and Problem Pregnancies, 2nd Edition Edited by SG Gabbe, JR Niebyl, JL Simpson. (1991)
Descent of the Breech Obstetrics - Normal and Problem Pregnancies, 2nd Edition Edited by SG Gabbe, JR Niebyl, JL Simpson. (1991)
Spontaneous Expulsion • spontaneous expulsion to the umbilicus • the sacrum should be gently guided anteriorly • singleton breech extraction is contraindicated • C/S is indicated for failure of descent or expulsion Obstetrics - Normal and Problem Pregnancies, 2nd Edition Edited by SG Gabbe, JR Niebyl, JL Simpson. (1991)
Hurry up & Wait! • DON’T PULL! • traction deflexes the fetal head • may cause nuchal arm Obstetrics - Normal and Problem Pregnancies, 2nd Edition Edited by SG Gabbe, JR Niebyl, JL Simpson. (1991)
Deliver Legs by lateral rotation of thighs and flexion of knees - keep sacrum anterior Obstetrics - Normal and Problem Pregnancies, 2nd Edition Edited by SG Gabbe, JR Niebyl, JL Simpson. (1991)
Delivery of Arms • good maternal pushing • deliver when winging of scapulae seen • rotate arm to anterior • sweep humerus across the chest and deliver • rotate other arm anterior and repeat to deliver Obstetrics - Normal and Problem Pregnancies, 2nd Edition Edited by SG Gabbe, JR Niebyl, JL Simpson. (1991)
Avoid Over-extension Obstetrics - Normal and Problem Pregnancies,2nd Edition Edited by SG Gabbe, JR Niebyl, JL Simpson. (1991)
Delivery of the head • Mauriceau - Smellie - Veit manoeuvre to deliver the head in flexion • The body should be supported in a horizontal position
Delivery of the head Obstetrics - Normal and Problem Pregnancies, 2nd Edition Edited by SG Gabbe, JR Niebyl, JL Simpson. (1991)
Delivery of the head • Forceps • assistant elevating babe • direct application Obstetrics - Normal and Problem Pregnancies, 2nd Edition Edited by SG Gabbe, JR Niebyl, JL Simpson. (1991)
Prevention of Breech • consider external cephalic version at 36 weeks gestation for eligible candidates • success rate 30 - 70% depending on experience • results in lower cesarean section rate
Conclusions • proper selection of patients • thorough explanation and informed consent • good progress in labour ( 0.5 cm/h after 3 cm) • induction and augmentation permissible • experienced attendants • standard fetal monitoring • assisted delivery - DON’T PULL - stay cool!