Download
1 / 86
880 likes | 1.15k Vues
Drugs for Reproductive Endocrinology: Focus on OCP therapeutics Ma. Stephanie Fay S. Cagayan, MD, FPOGS. General Objective. To acquire an understanding of the action of the different sex hormones and other hormones utilized in the pharmacology of hormonal contraception

E N D
Drugs for Reproductive Endocrinology: Focus on OCP therapeutics Ma. Stephanie Fay S. Cagayan, MD, FPOGS
General Objective To acquire an understanding of the action of the different sex hormones and other hormones utilized in the pharmacology of hormonal contraception Reference: Chapter 40, Basic and Clinical Pharmacology 1th edition (Katzung)
Specific Objectives To be able to review the physiology of normal menstrual cycle To list the different sex hormones, know their biosynthesis (chemical compositions), mechanism of action, pharmacokinetic properties, physiologic and metabolic effects To describe clinical/therapeutic applications of these hormones To list side effects and/or adverse reactions to these drugs
Outline Physiology of Reproductive Hormones Female Gonadal Hormones Estrogen and Progesterone ORAL CONTRACEPTION
Different Hormones in Reproductive Endocrinology Biosynthesis (chemical compositions) Mechanism of action Pharmacokinetic properties Physiologic and Metabolic effects Clinical / Therapeutic Application Adverse Effects
Outline Physiology of Reproductive Hormones Female Gonadal Hormones Estrogen and Progesterone ORAL CONTRACEPTION
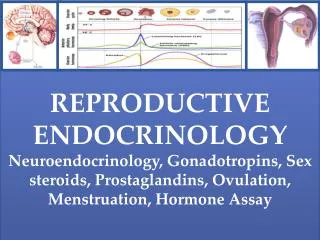
Sex hormones = gonadal hormones estrogens progestins androgens Gonadotropins LH FSH GnRH
Gonadal Hormones SYNTHESIS OF SEX STEROIDS
Gonadal Hormones SEX HORMONES: 21 carbon series – PROGESTINS (pregnane nucleus) 19 carbon series - ANDROGENS (androstane nucleus) 18 carbon series - ESTROGENS (estrane nucleus) What regulates the synthesis of sex hormones?
Hypothalamic-Pituitary-Reproductive Axis: TWO CELL-SYSTEMS (Testosterone) (Androstenedione)
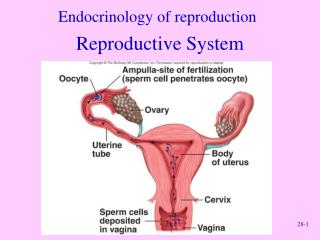
Prerequisites of Normal Menstruation an intact HPO axis estrogen-induced proliferative endometrium ovulation at midcycle progesterone-induced secretory endometrium if pregnancy does not occur, the hormones decline, and withdrawal bleeding occurs
Major natural estrogens in human Actions mediated by ESTROGEN RECEPTORS (alpha and beta) which are ligand-regulated transcription factors The Estrogens
The Estrogens Biosynthesis (chemical compositions) Mechanism of action Pharmacokinetic properties Physiologic and Metabolic effects Clinical / Therapeutic Application Adverse Effects
Estrogen Receptor Actions mediated by ESTROGEN RECEPTORS (alpha and beta) which are ligand-regulated transcription factors
The Estrogens: Pharmacokinetics Estradiol (E2) binds STRONGLY to α globulin (SHBG) LOWER affinity to albumin E2 (liver) → Estrone (E1) and Estriol(E3) → hydroxylated derivatives and conjugated metabolites Orally administered estrogens have HIGH ratio of hepatic to peripheral effects → responsible for the increased clotting factors and increased renin substrate
Clinical / Therapeutic Application Primary hypogonadism Hormonal contraception Post-menopausal hormonal therapy
The Estrogens Biosynthesis (chemical compositions) Mechanism of action Pharmacokinetic properties Physiologic and Metabolic effects Clinical / Therapeutic Application Adverse Effects
Adverse Effects Uterine bleeding Endometrial cancer Other effects: nausea, breast tenderness
The Natural Progestins: Progesterone • The most important progestin in human • Serves as a precursor to the estrogens, androgens and adrenocortical steroids • Synthesized in the ovary, testis and adrenal from circulating cholesterol; large amounts are also synthesized and released by the placenta during pregnancy
The Synthetic Progestins 21 carbon compounds 19-nor, 13 ethyl compounds Hydroxyprogesterone acetate Medroxyprogesterone acetate Megestrol Dimethisterone * Most closely related to progesterone Desogestrel Gestodene Norgestimate ** claimed to have lower androgenic activity than older synthetic progestins
Actions are mediated by progesterone receptors (A and B isoforms) which are ligand-activated transcription factors The concentration of progesterone receptors is dependent on previous estrogen action The Progestins
The Progestins Biosynthesis (chemical compositions) Mechanism of action Pharmacokinetic properties Physiologic and Metabolic effects Clinical / Therapeutic Application Adverse Effects
The Progestins: Pharmacokinetics Progesterone is rapidly absorbed following administration by any route t ½ is 5minutes Almost completely metabolized in one passage through the liver In the liver, it is metabolized to pregnanediol and conjugated with glucuronic acid It is excreted into the urine as pregnanediol glucuronide
The Progestins Biosynthesis (chemical compositions) Mechanism of action Pharmacokinetic properties Physiologic and Metabolic effects Clinical / Therapeutic Application Adverse Effects
Physiologic Effects • Decreases amount of cervical mucus and increases its viscosity • Increases basal body temperature Promote endometrial development during luteal phase
Progesterone ATTENUATES estrogen action on the endometrium in 3 ways: The Physiologic Effect of Progestins By reducing the rate of synthesis of ER molecules By increasing the rate of enzymatic inactivation By effecting estrogen inactivation through sulfuration
Physiologic Effects: Progesterone Has little effect on protein metabolism Has more marked effect on carbohydrate metabolism: progesterone INCREASES basal insulin levels and the insulin response to glucose Antagonize actions of aldosterone
Physiologic Effects: Progesterone Increases body temperature Has depressant and hypnotic effects on the brain Increases ventilatory response to CO2 Stimulate growth and development of breasts during pregnancy Its effects on the uterus are essential for maintenance of pregnancy
Clinical Application THERAPEUTIC APPLICATION: Hormonal contraception Hormonal replacement therapy Endometriosis
Clinical Application: D I A G N O S T I C A test of estrogen secretion: Progesterone challenge test - MPA 10mg/d for 5 days - when endometrium has been stimulated by estrogens (+) withdrawal bleeding
Adverse Effects Headache Dizziness Bloating Weight gain Reversible reduction of glucose tolerance
Hormonal contraception in women Combination of progestins and estrogens – Combination oral contraceptives (COCs) Progestin only pills (POPs)
The Pharmacology of the Estrogen Component of COCs E2 is the most potent natural estrogen --- inactive orally E2 + ethinyl group at the 17 position = Ethinyl Estradiol --- orally active
The Pharmacology of the Estrogen Component of COCs Metabolism of EE VARIES SIGNIFICANTLY from individual to individual, and from one population to another ESTROGEN CONTENT of the pill is of major clinical importance ---- THROMBOSIS is dose-related DOSE OF ESTROGEN – a critical issue in selecting an oral contraceptive
COMBINATION ORAL CONTRACEPTIVES (COCS) – PROGESTIN COMPONENT 42
The Pharmacology of the Progestin Component of COCs 2 major types of synthetic progestins Derivatives of 19 nortestosterone Derivatives of 17α acetoxyprogesterone
The Pharmacology of the Progestin Component of COCs NORETHINDRONE ETHISTERONE TESTOSTERONE Removal of 19-carbon from ethisterone formed NORETHINDRONE → changed major hormonal effect from an androgen to progestational agent → 19 nortestosterone - all progestational agents have some degree of androgenic activity
The Pharmacology of the Progestin Component of COCs 19 NORTESTOSTERONE ESTRANES Norethindrone Norethynodrel Norethindrone acetate Ethynodiol acetate GONANES Levonorgestrel Norgestimate* Gestodene* Desogestrel* * With greater progestational activity
The Pharmacology of the Progestin Component of COCs Other progestins • Levonorgestrel is the active isomer of norgestrel New progestins • Desogestrel, gestodene, norgestimate are derivatives of levonorgestrel • Reduced androgenicity (increased sex hormone binding globulin, decreased free testosterone) • Drospirenone – analogue of spironolactone, has affinity for mineralocorticoid receptor and antimineralocorticoid effect (Yasmin)
The Pharmacology of the Progestin Component of COCs 17 α ACETOXYPROGESTERONE C21 progestins PREGNANES Structurally related to progesterone Medroxyprogesterone acetate and megestrol acetate Marketed for noncontraceptive usage
COCs “ Current formulations of COCs are made from SYNTHETIC steroids and contain no natural estrogens or progestins.”
syntheticprogestins Ethinyl estradiol
Definitions Low Dose Oral Contraceptives – products with <50ug of EE 1st generation COCs – products with > 50ug of EE 2nd generation COCs – products with levonorgestrel,norgestimate, and other members of the norethindrone family and <50ug EE 3rd generation COCs – products with desogestrel or gestodene and <50ug of EE