Olecranon fractures
390 likes | 994 Vues
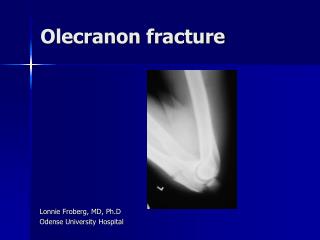
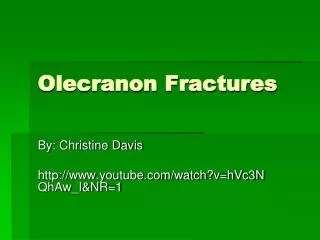
Olecranon fractures. Goran Milovic MRT North Shore Hospital (WDHB). Introduction.

Olecranon fractures
E N D
Presentation Transcript
Olecranon fractures Goran Milovic MRT North Shore Hospital (WDHB)
Introduction • Approximately 10% of fractures, about the adult elbow, consist of fractures of the olecranon process of the ulna. The fractures range from simple non displaced fractures to complex fractures /dislocations of the elbow (Buijze & Kloen, 2009; Veillette & Steinmann, 2008). • In this presentation we will look at fractures of the olecranon, treatment options, possible complications of those treatments and some issues regarding the reporting of the post operative images.
Incidence and demographics • There is no data linking olecranon fractures to specific age group, sex or race. • There is no data linking olecranon fractures to particular disease or syndrome. • There is no data linking olecranon fractures to any specific activity (including extreme sports and gardening).
Imaging of the elbow • The standard anterioposterior (AP) and true lateral x-ray images of the elbow are sufficient for evaluation of the isolated olecranon fracture (Hak & Golladay, 2000). • Poorly aligned images, or images in a splint are not well suited for accurate diagnosis, classifying the fracture and formal preoperative planning (Veillette & Steinmann, 2008). • The general opinion among reviewed authors is that plain x-ray imaging is sufficient for initial diagnosis of the olecranon fractures and more advanced imaging modalities (MRI, CT) should be only used in cases of complex elbow injuries.
Mechanism of injury and Associated injuries • Most olecranon fractures result from a fall with direct trauma to the olecranon or landing on the outstretched hand with eccentric contraction of the triceps during resisted elbow flexion. • Olecranon fractures are usually isolated injuries but in cases of politrauma or high energy trauma ipsilateral extremity injuries should be carefully assessed as associated fractures of the coronoid process or radial head and Monteggia fracture-dislocations have a significant impact on elbow stability (Hak & Golladay, 2000).
Case Study Patient history • A 81 year old female presented to emergency department of the North Shore Hospital with history of being knocked over by a car and with gross swelling / haematoma of the posterior aspect of the left elbow. • The AP and lateral x-rays of the left elbow demonstrated a fractured olecranon.
Case Study Initial images • The AP image of the elbow was not of sufficient diagnostic value, with the performing MRT failing to adapt the technique to correctly demonstrate joint and bony anatomy of the elbow. However, the lateral image was sufficient to diagnose an olecranon fracture. (WDHB Image bank)
Case Study • The initial images were reported as: “There is diffuse swelling principally about the proximal ulna where there is a displaced fracture through the olecranon process by approximately 1 cm. It is slightly retracted along the posterior surface of the humerus. No other definite fracture is seen”
Case Study Theatre images • The patient was sent to theatre for open reduction and internal fixation. Tension band wire technique was used as a means of internal fixation. • Radiologist report states that: “Two image intensifier views taken in theatre following internal fixation of a comminuted olecranon fracture with two Kirschner wires (K-wires) and figure of 8 wire in situ maintaining alignment. Alignment post fixation appears near anatomical with no complication demonstrated.” • The performing orthopaedic surgeon noted in the post operative report that: “The image intensifier revealed one of the wires had failed to re-engage the distal cortex. This was accepted at this stage.”
Case Study (WDHB Image bank)
Case Study First follow up images • Approximately six weeks later patient returned to the Orthopaedic clinic for follow up and new AP and lateral images were taken. • The reporting radiologist noted that: “Left elbow K- wires and a tension band internally fix the comminuted olecranon fracture. Alignment is near anatomical and unchanged compared with intra operative images from 21 October 2009.” • Comments entered in clinical notes by the orthopaedic surgeon are similar to the radiologist findings but without mentioning any comminution of the fracture.
Case Study (WDHB Image bank)
Case Study Second follow up images • The patient returned to the Orthopaedic clinic four weeks later for the final follow up with a new set of x-rays taken and radiologist reporting: “Alignment at the olecranon fracture traversed by K- wires and tension band wiring is unchanged from the prior film. The fracture remains faintly visible.” • The orthopaedic surgeon agreed with radiologist report in regard of the fracture status but had more comments on the status of the surgical hard ware, stating:” X-ray taken of the elbow shows the fracture to be going onto unite satisfactorily. One of the longitudinal wires has backed out and is sitting under the skin. This lady has done very well following her fracture, however one of her wires is starting to back out. This is causing some pressure on the overlying skin, this is not broken down.”
Case Study (WDHB Image bank)
Review of the findings by the reporting radiologists and orthopaedic surgeon • All the reports were from different radiologists and from different orthopaedic consultants and registrars • As we can see from the comparison, two out of four radiology reports are failing to mention incorrect position or changes in position of the K-wires and in two of the reports there is diagnosis of the comminution not seen on the initial images or intra operatively. • The reports from the radiologist had no influence on the patient management and outcome of the treatment received by the patient.
Review of the findings by the reporting radiologists and orthopaedic surgeon The questions arising from this findings could be: 1. Should radiologists report plain orthopaedic imaging at all, exception being initial imaging? 2. Is there room for some other imaging professionals, MRT’s namely, to report plain orthopaedic images only? Perhaps the answers to these questions could be the subject of the some focused and more in depth study.
Treatment of the olecranon fractures • The severity of the fracture, concomitant elbow trauma and ligamentous instability will influence surgical decision making and outcome (McKay & Katarincic, 2002). • There are two different opinions on the treatment of the undisplaced intra articular fractures with (Buijze & Kloen, 2009; Hak & Golladay, 2000; Rommens, Küchle, Schneider, & Reuter, 2004) advocating operative treatment as the only option to restore anatomy and joint stability of the elbow. • The proponents of non operative treatment (Hak & Golladay, 2000; Veillette & Steinmann, 2008) are stating that non displaced fractures of the olecranon can be successfully managed by immobilisation only, with same rate of success as operative treatment but with no post operative complications.
Treatment of the olecranon fractures • There are several treatment options for internal fixation of the olecranon fractures: • Tension-band wiring • Plate fixation • Triceps advancement after fragment excision. • The method of internal fixation is chosen primarily on fracture type (Veillette & Steinmann, 2008).
Tension band wiring • Tension band wiring technique is a method recommended by the Arbeitsgemeinschaft für Osteosynthesefragen group (Orthopaedic Trauma Association - AO group) for non comminuted transverse fractures of the olecranon (Mullett, et al., 2000). • Multyfragmentary fractures cannot be fixed with a tension band. In order to be able to use a tension band, the anterior cortex cannot be comminuted (AO group, K.Kojima&S.Velkes) • Union rates and elbow function after tension band fixation are very good or excellent in the majority of patients (Holdsworth & Mossad, 1984). • The tension band wire construct converts the tensile distraction force of the triceps into a dynamic compressive force across the olecranon articular surface (Veillette & Steinmann, 2008)
Tension band wiring • The tensile distraction force-“pulling force” of the triceps is perhaps best illustrated on the lateral view of the elbow. • The lateral image with K-wires and tension band wiring in place shows how those forces of the triceps muscle can be used to compress fracture in a anatomical position. • Rockwood & Green’s Fractures in Adults
Tension band wiring (WDHB Image bank)
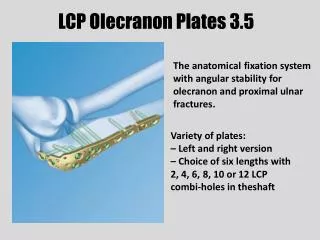
Plate fixation • Biomechanical and clinical studies demonstrate plate fixation to be superior to tension band wiring when significant comminution is present (McKay & Katarincic, 2002). • The plate fixation method is also indicated for oblique fractures distal to the midpoint of the trochlear notch, fractures that involve the coronoid process and those associated with Monteggia fracture-dislocation of the elbow (Hak & Golladay, 2000). • Using a plate has several advantages as the plate allows improved contouring and can be appropriately placed on the dorsal tension surface of the proximal ulna, around the tip of olecranon, to help hold the proximal fragment when poor bone quality limits screw placement (Veillette & Steinmann, 2008)
Plate fixation (Buijze & Kloen, 2009, p. 2418)
Excision of fragment and triceps advancement • This method is usually indicated in elderly patients with severely comminuted fracture or the olecranon fracture where fragments are too small and internal fixation would not be successful (Veillette & Steinmann, 2008). • The method involves the excision of the fracture fragments thru the incision and reattachment of the triceps tendon close to articular surface (Gartsman, Sculco, & Otis, 1981). • Excision of fragment and triceps advancement can be used as a salvage procedure if internal fixation fails (Hak & Golladay, 2000).
Excision of fragment and triceps advancement (Veillette & Steinmann, 2008, p. 5)
Excision of fragment and triceps advancement (Veillette & Steinmann, 2008, p. 5)
Prognosis and Complications • Prognosis after olecranon fractures are generally good to excellent, with most studies noting satisfactory outcomes and restoration of the normal or near –normal function in more than 95% of the patients (Veillette & Steinmann, 2008). • However, Rommens, et al. (2004, p.192) reports infection, delayed union and ulnar nerve palsy as complication in up to 10% of the cases. • Hardware prominence and painful irritation requiring removal is the most frequent complication after internal fixation of the olecranon fracture (Hak & Golladay, 2000). The same authors reported that up to 80% of the post operative complaints related to symptomatic hardware prominence.
Prognosis and Complications • Rommens, et al. (2004, p.196) advocated the hardware removal after fracture healing and states that “functional deficits in the activities of daily life were more than twice as frequent before than after hardware removal.” • Loss of motion is a common problem after fractures of the elbow but it is usually insignificant in patients with olecranon fractures. • Patients with isolated olecranon injuries typically lose 10⁰ to 15⁰of extension but this is considered to be minor (Hak & Golladay, 2000). • Early initiation of the motion is one of the imperatives of the rehabilitation process. The ideal time for early motion is not determined by most authors but as early as day one has been suggested (Hak & Golladay, 2000).
Case Study Outcome • The outcome of the surgical treatment and rehabilitation were favourable to the patient. Protruding K-wire didn’t affect outcome of the ostheosynthesis and the performing orthopaedic surgeon was satisfied with the fracture healing and patient progression post surgery. • The need to remove one of K-wires was recognized as one of potential complications explained to the patient prior to surgery and once the wire was removed patient continued to use elbow freely with minimal restrictions in the range of the movement.
Conclusion • Olecranon fractures are commonly seen in every day practice of MRT’s working in the emergency departments. • Good initial films are essential for the accurate diagnosis and preoperative planning with correct AP and true lateral film as a must. • Plain films are also used for the post operative imaging and in most cases they are sufficient to follow up the progression of the healing process and to assure correct position of the surgical hardware.
Conclusion • As mentioned earlier there are several surgical techniques used to treat olecranon fractures. Those techniques are well established with characteristic appearances of orthopaedic hardware on post operative images. • Accordingly, this could raise the question of why such obvious and easily seen malfunction of the orthopaedic hardware has been overlooked by highly skilled and very experienced radiologists? • This case study was used to highlight this issue, together with attempt of summarising the olecranon fractures, their treatment and outcomes of the treatment.
References • Bryce, C. D., & Armstrong, A. D. (2008). Anatomy and Biomechanics of the Elbow. The Orthopedic clinics of North America, 39(2), 141-154.[Online]. Available: http://www.orthopedic.theclinics.com/issues/contents?issue_key=S0030-5898%2808%29X0002-1 • Buijze, G., & Kloen, P. (2009). Clinical Evaluation of Locking Compression Plate Fixation for Comminuted Olecranon Fractures. J Bone Joint Surg Am, 91(10), 2416-2420. • Daniels, D. L., Mallisee, T. A., Erickson, S. J., Boynton, M. D., & Carrera, G. F. (1998). The elbow joint: osseous and ligamentous structures. Radiographics, 18(1), 229-236. • Gartsman, G., Sculco, T., & Otis, J. (1981). Operative treatment of olecranon fractures. Excision or open reduction with internal fixation. J Bone Joint Surg Am, 63(5), 718-721. • Greenspan, A. (2004), Othopaedic imaging: A practical approach(4th ed), Chicago, Lippincott,Williams & Wilkins. • Hak, D. J., & Golladay, G. J. (2000). Olecranon Fractures: Treatment Options. J Am Acad Orthop Surg, 8(4), 266-275.[Online].Available: http://www.jaaos.org/cgi/content/abstract/8/4/266 • Holdsworth, B. J., & Mossad, M. M. (1984). Elbow function following tension band fixation of displaced fractures of the olecranon. Injury, 16(3), 182-187. [Online]. Available: http://www.springerlink.com/content/t34242r078g72245/ • Kuntz, D. G., & Baratz, M. E. (1999). FRACTURES OF THE ELBOW. The Orthopedic clinics of North America, 30(1), 37-61. [Online]. Available: http://www.orthopedic.theclinics.com/article/S0030-5898(05)70060-2/abstract • Macko, D., & Szabo, R. (1985). Complications of tension-band wiring of olecranon fractures. J Bone Joint Surg Am, 67(9), 1396-1401.
References • McKay, P. L., & Katarincic, J. A. (2002). Fractures of the proximal ulna olecranon and coronoid fractures. Hand clinics, 18(1), 43-53. • Morrey, B., Askew, L., & Chao, E. (1981). A biomechanical study of normal functional elbow motion. J Bone Joint Surg Am, 63(6), 872-877. • Morrey, B. F. (1995). Current Concepts in the Treatment of Fractures of the Radial Head, the Olecranon, and the Coronoid. J Bone Joint Surg Am, 77(2), 316-327. • Mullett, J. H., Shannon, F., Lawlor, G., Lee, T. C., & Rourke, S. K. (2000). K-Wire position in tension band wiring of the Olecranon ,A comparison of two techniques. Injury, 31(6), 427-431. [Online]. Available: http://www.injuryjournal.com/article/S0020-1383(00)00014-0/abstract • Prasad, A., Robertson, D. D., Sharma, G. B., & Stone, D. A. (2003). Elbow: The Trochleogingylomoid Joint. Semin Musculoskelet Radiol, 07(01), 019-026. [Online].Available: http://www.ncbi.nlm.nih.gov/pubmed/12888941 • Rommens, P. M., Küchle, R., Schneider, R. U., & Reuter, M. (2004). Olecranon fractures in adults: factors influencing outcome. Injury, 35(11), 1149-1157. [Online].Available: http://www.injuryjournal.com/article/S0020-1383(03)00525-4/abstract • Schenk, M., & Dalinka, M. K. (1997). IMAGING OF THE ELBOW: An Update. The Orthopedic clinics of North America, 28(4), 517-535. [Online]. Available: http://www.mdconsult.com/das/article/body/187850032-2/jorg=journal&source=&sp=9965631&sid=0/N/104822/1.html?issn=00305898 • Veillette, C. J. H., & Steinmann, S. P. (2008). Olecranon Fractures. The Orthopedic clinics of North America, 39(2), 229-236. [Online]. Available: http://www.mdconsult.com/das/article/body/187850032-2/jorg=journal&source=&sp=20555569&sid=0/N/636210/1.html?issn=00305898 • WDHB Image bank. (2010). Images of the case study patient accessed on 12/12/2009 & 15/2/2010