Fractures and Mobility Issues
Learn about fractures, common causes, classifications, pathophysiology, diagnosis, treatment, and bone healing in this informative guide.

Fractures and Mobility Issues
E N D
Presentation Transcript
Fractures and Mobility Issues Nurs 120 Sasha A. Rarang, RN, MSN
Bones • There are about 206 bones in the adult body. • Bones are made up dense connective tissue • Used for mineral storage, protection, support, and movement, ect.
Fractures • Is a discontinuity of the bone and is the most common type of bone lesion. • Occur when more stress is placed on the bone than it is able to absorb. • Grouped according to cause, fractures can be divided into three major categories: • Fractures caused by sudden injury (most common) • Fatigue or stress fractures • Pathologic fractures (Osteoporosis related)
Common Causes of Injury • High-speed motor accidents in adults younger than 45 years of age • Childhood injuries due to falls, bicycle-related injuries, and sports injury • Falls are the most common cause of injury in people 65 yeas of age and older, with fractures of the hip and proximal humerus particularly common in this age group.
Pathophysiology • The musculoskeletal system includes the bones, joints, and muscles of the body together with associated structures such as ligaments and tendons. • This system which constitutes more than 70% of the body, is subject to a large number of disorders. • These disorders affect persons in all age groups and walks of life and are a major cause of pain and disability.
Continued… • A broad spectrum of musculoskeletal injuries results from numerous physical forces, including blunt tissue trauma, disruption of tendons and ligaments, and fractures of bony structures. • Many of the forces that cause injury to the musculoskeletal system are typical for a particular environmental setting, activity, or age group.
Classifications • Fractures are classified according to location, type, and direction or pattern of the fracture line. • Location; A fracture of the long bone is described in relation to its position in the bone- proximal, midshaft, and distal. • Direction: Transverse, oblique, or spiral • Type: Comminuted, segmental, butterfly, or impacted.
Classifications continued… • Other descriptions are used when the fracture affects the head or neck of a bone, involves a joint, or is near a prominence such as a condyle or melleoulus. • Fractures are determined by its communication with the external environment, the degree of break in continuity of the bone, and the character of the fracture pieces. • A fracture can be classified as open or closed, depending if the bone fragments have broken through the skin
Sudden Injury Fractures • The force causing the fracture may be direct, such as a fall or blow, or indirect, such as a massive muscle contraction or trauma transmitted along the bone
Fatigue Fracture • Results from repeated wear on a bone. • Pain associated with overuse injuries of the lower extremities, especially posterior medial tibial pain, is one of the most common symptoms that physically active persons, such as runners, experience.
Pathologic Fracture • Occurs in bones that already are weakened by disease or tumors. • May occur spontaneously with little or no stress. • The underlying disease state can be local, as with infections, cysts, or tumors, or it can be generalized, as in osteoporosis, Paget disease, or disseminated tumors.
Diagnosis and Treatment • Diagnosis is the first step in the care of fractures and is based on history and physical manifestations. • X-ray examination is used to confirm diagnosis and direct the treatment • Treatment depends on the general condition of the person, the presence of associated injuries, the location of the fracture, and its displacement, and whether the fracture is opened or closed. • A splint is a device for immobilizing the movable fragments of a fracture; the injured part should always be splinted before it is moved. This is essential for prevention of further injury.
Three Objectives for Treatment of Fractures • Reduction of the fracture; is directed toward replacing the bone fragments to as near-normal an anatomic position as possible. • Immobilization; prevents movement of the injured parts and is the single most important element in obtaining union of the fracture fragments. Can be accomplished with the use of external devices such as splints, casts, external fixation devices, or traction, or by reduction. • Preservation and restoration of the function of the injured part; this is an ongoing process that includes unaffected and affected extremities during the period of immobilization. Exercises designed to preserve function, maintain muscle strength, and reduce joint stiffness should be started early.
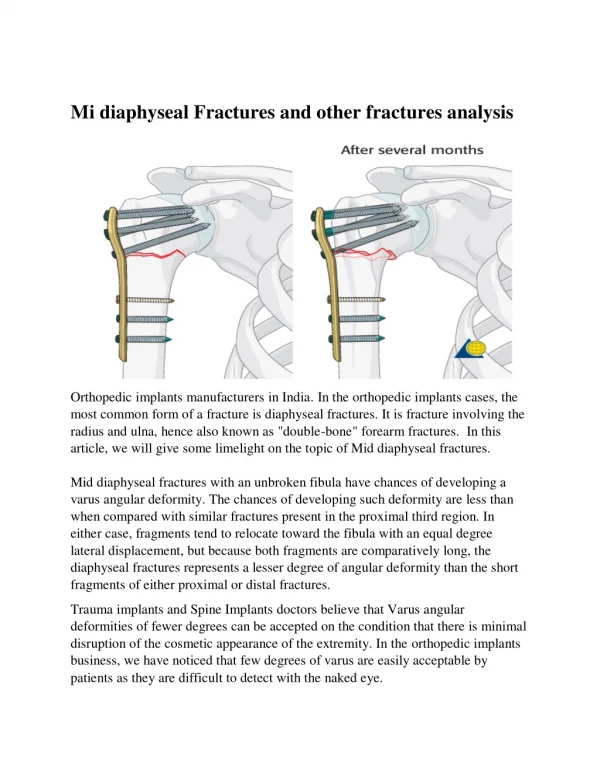
Bone Healing • There are essentially four stages involved in bone healing: Hematoma formation, fibrocartilaginous callus development, ossification, and remodeling. • The degree of the response during each of these stages is in direct proportion to the extent of trauma. • Healing time depends on the site of the fracture, the condition of the fracture fragments, hematoma formation, and other local and host factors. • 4-6 Weeks in adolescents and 10-18 weeks for adults. • Function usually returns within 6 months after union is complete, but may also take longer.
MANIFESTATIONS:GENERAL SIGNS AND SYMPTOMS • Pain • Tenderness • Swelling • Loss of function • Deformity • Immobility • Neurological damage (Numbness, loss of sensation) • Loose muscles and muscle spasms
Manifestations continued… • A crepitus or grating sound may be heard as the bone fragments rub against each other. • In the case of an open fracture, there is bleeding from the wound where the bone protrudes. • Blood loss from a pelvic fracture or multiple long bone fractures can cause hypovolemic shock in a trauma victim • Nerve function at a fracture site may be temporarily lost. • Numbness in the area and surrounding muscles may become flaccid, this is called local shock. This may last from several minutes to an hour and after his brief period, the pain sensation returns and, with it, muscle spasms and contractions of the surrounding muscles.
DEFORMITIES OF LONG BONE FRACTURES • Angulation • Felt at the site and is pushed up against soft tissues producing a tenting effect • Shortening • Bone fragments that slide and overridge each other b/c of the pull of muscles on the long axis of the extremity. • Rotation • Fracture fragments rotate out of their longitudinal axis resulting from rotational strain produced by the fracture or unequal pull by muscles that are attached to the fracture fragments
HUMERUS FRACTURES • Radial nerve injury (loss of sensation • Vascular injury to the brachial artery • Results from fracture and may cause laceration and muscle spasm • Pain, inability, bruising, swelling, numbness and weakness of the arms and wrists • Deformities may occur at the shoulders, upper arms, elbows
PELVIC BONE FRACTURES • May cause intraabdominal injuries • Paralytic ileus • Hemorrhage and laceration of urethra, bladder and colon • Local swelling • Tenderness • Deformity • Unusual pelvic movement • Ecchymosis (discoloration of the skin from bleeding underneath) on the abdomen • Pelvic, back, hip and leg pain • Difficulty walking
PELVIC BONE FRACTURES (CONT) • Severe symptoms include: • Heamturia • Dizziness and fainting • Leg numbness and weakness
HIP FRACTURES • Muscle spasms • Shortening of affected extremity • Severe pain and tenderness • Hip, groin, lower back, suprapubic area, knee • Hip swelling • Walking with a limp • Inability to stand • Leg numbness and weakness
FEMORAL FRACTURES • Common in young adults • May appear deformed, angulated, shortened • Pain around thighs • Inability to perform ROM w/ hip or leg • Fat embolism (series of symptoms that include petechial skin rash, respiratory failure and cerebral dysfunction due to the presence of fat droplets in small blood vessels as a result of a long bone fracture or major trauma) • Nerve and vascular injury • Soft tissue damage • Problems associated w/ bone unity
TIBIA FRACTURES • Fat Embolism • Problems w/ bone unity • Possible infection w/ open fracture • Compartment syndrome (the compression of nerves and blood vessels within an enclosed space that results in muscles and nerve damage and problems w/ blood flow) • Pain • Swelling • Bruising • Deformity • Numbness • Weakness
VERTEBRAL FRACTURE • Damage to spinal cord (serious problem) • Critical nerve damage • Pinched nerves • Paralysis and even death • In osteoporosis PTs w/ vertebral fractures, several vertebras are involved because of the Dowager’s hump • Bowel and bladder dysfunction • Indication of disruption of the ANS nerves or injury to spinal cord • Symptoms include bowel and bladder incontinence • Spine curved forward • Back stiffness and back pain that worsens w/ movement
FACIAL FRACTURES • Frontal Bone • Rapid edema that may hide underlying fractures • Perioorbital bone • Possible frontal sinus and ocular muscle involvement, putting the ocular muscles at risk of being damaged • Nasal bone • Dislocate the nasal bones and bleeding may follow • Zygomatic arch • Depression of the zygomatic arch and ocular muscles at risk of being damaged • Maxilla • Segmental motion of maxilla and alveolar fracture of teeth • Mandible • Tooth fractures, bleeding, limited motion of mandible
Nursing Process Assessment: S&S: Pain, swelling, and tenderness. Can be from a traumatic injury, stress or long term repetitive force to a site, disease, immobility for a certain amount of time, osteopenia, and osteoporosis. Medications like corticosteroids for long term use create chances for fracture. You may also notice a deformity at fracture site, skin lacerations, pallor and cool skin or bluish and warm skin, muscle weakness, or crackling between two broken bones (crepitus). The extent of the fracture can be seen on x-rays, bone scans, CT scans, or MRI.
Diagnosis: Impaired physical mobility related to loss of integrity of bone structures, acute pain and associated with reluctance to move, bone fragment movement, injury of soft tissue, risk for peripheral neurovascular dysfunction, disruption of skin integrity, limited movement restrictions as seen by limited joint range of motion, inability to intentionally move, and inability to bear weight. Planning: Patient will have physiologic healing with no complications, return of skeletal function, maintenance and realignment by immobilization, will demonstrate appropriate use of cast or immobilizer, obtain pain relief, and will achieve maximum rehabilitation potential.
Nursing Management Implementation: • Neurovascular assessment of fractured extremity for any changes. Check pulse, for edema, color, temperature. • Minimize pain by proper alignment , support of extremity, and positioning of patient. • Keep extremity elevated above heart. • Look at dressing or casts to monitor for bleeding and look over bony prominences for skin integrity. • Fractured mandible: Check for patent airway, maintain clean oral hygiene, and adequate nutrition.
Nursing Management : Cont. • Because of limited movement, to prevent constipation, maintain a high fluid intake and fibrous foods. • Offer information on cast care and how to recognize complications. • Assist patient with ambulation to help determine the patient’s abilities. Give referrals to long term rehabilitation programs. • Fractured hip: keep hip in neutral position when sitting, walking, or laying down. • Fractured humerus: Protect the axilla of skin breakdown due to constant sweating with absorption pads.
Nursing Management Evaluation: • Patient’s pain alleviated through proper positioning and alignment. • Pt is compliant with diet changes and understands the need for long term rehabilitation.
Question #1 What constitutes a fracture?
Question #2 What are the common causes of injury? Name at least two.
Questions #3 A fracture in which the line of break runs obliquely to the axis of the bone is an example of? • Displaced fracture • Stress fracture • Greenstick fracture • Oblique fracture
Questions #4 When you using a cane, the most important thing to remember is? • Use cane to hit the nurse to get her attention • 2 point gait • Using the cane on your weak side • Using the cane on your strong side
Question #5 In identifying people at risk for fractures, the nurse recognizes that the person at greatest risk for impacted fracture is • A female client over 40 years old walking her dog • A 21 year old male who plays basketball 6 times a week for 6 hours • A 5 year old male playing at the playground • A 90 year old female with a history of falls