Download
1 / 1
10 likes | 452 Vues
Multifocal Myxopapillary Ependymoma : A Case Report 1 Joseph R. Grajo, M.D., 2 Gitasree Borthakur , B.S., 1 Natasa Dragicevic , M..D., Ph.D., 3 Thora Steffensen , M.D., 1 Gregg Baran , M.D ., F.A.C.R 1 University of South Florida, Department of Radiology, Tampa, FL

E N D
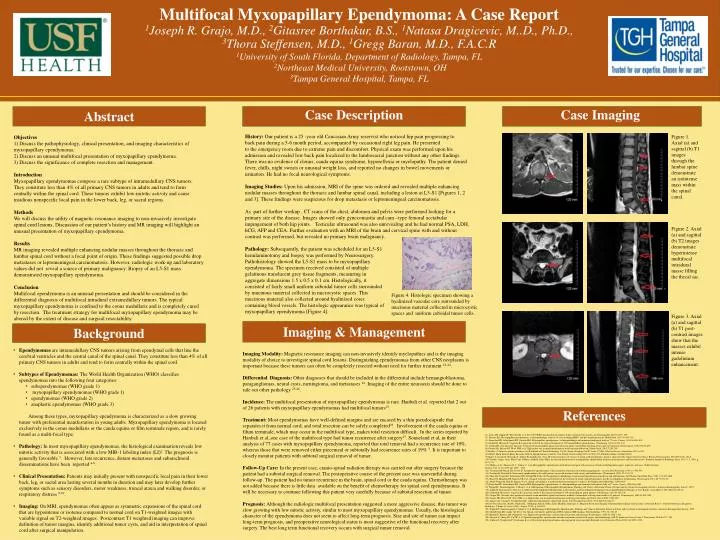
Multifocal MyxopapillaryEpendymoma: A Case Report 1Joseph R. Grajo, M.D., 2Gitasree Borthakur, B.S., 1Natasa Dragicevic, M..D., Ph.D., 3Thora Steffensen, M.D., 1Gregg Baran, M.D., F.A.C.R 1University of South Florida, Department of Radiology, Tampa, FL 2Northeast Medical University, Rootstown, OH 3Tampa General Hospital, Tampa, FL Case Imaging Abstract Case Description History: Our patient is a 25 -year old Caucasian Army reservist who noticed hip pain progressing to back pain during a 5-6 month period, accompanied by occasional right leg pain. He presented to the emergency room due to extreme pain and discomfort. Physical exam was performed upon his admission and revealed low back pain localized to the lumbosacral junction without any other findings. There was no evidence of clonus, caudaequina syndrome, hyporeflexia or myelopathy. The patient denied fever, chills, night sweats or unusual weight loss, and reported no changes in bowel movements or urination. He had no focal neurological symptoms. Imaging Studies: Upon his admission, MRI of the spine was ordered and revealed multiple enhancing nodular masses throughout the thoracic and lumbar spinal canal, including a lesion at L5-S1 [Figures 1, 2 and 3]. These findings were suspicious for drop metastasis or leptomeningealcarcinomatosis. As part of further workup , CT scans of the chest, abdomen and pelvis were performed looking for a primary site of the disease. Images showed only gynecomastia and cam –type femoral acetabular impingement of both hip joints. Testicular ultrasound was also unrevealing and he had normal PSA, LDH, hCG, AFP and CEA. Further evaluation with an MRI of the brain and cervical spine with and without contrast was performed, but revealed no primary brain malignancy. Figure 1. Axial (a) and sagittal (b) T1 images through the lumbar spine demonstrate an isointensemass within the spinal canal. Objectives 1) Discuss the pathophysiology, clinical presentation, and imaging characteristics of myxopapillaryependymoma. 2) Discuss an unusual multifocal presentation of myxopapillaryependymoma. 3) Discuss the significance of complete resection and management. Introduction Myxopapillaryependymomas compose a rare subtype of intramedullary CNS tumors. They constitute less than 4% of all primary CNS tumors in adults and tend to form centrally within the spinal cord. These tumors exhibit low-mitotic activity and cause insidious nonspecific local pain in the lower back, leg, or sacral regions. MethodsWe will discuss the utility of magnetic resonance imaging to non-invasively investigate spinal cord lesions. Discussion of our patient’s history and MR imaging will highlight an unusual presentation of myxopapillaryependymoma. ResultsMR imaging revealed multiple enhancing nodular masses throughout the thoracic and lumbar spinal cord without a focal point of origin. These findings suggested possible drop metastases or leptomeningealcarcinomatosis. However, radiologic work-up and laboratory values did not reveal a source of primary malignancy. Biopsy of an L5-S1 mass demonstrated myxopapillaryependymoma. ConclusionMultifocal ependymoma is an unusual presentation and should be considered in the differential diagnosis of multifocal intraduralextramedullary tumors. The typical myxopapillaryependymoma is confined to the conusmedullaris and is completely cured by resection. The treatment strategy for multifocal myxopapillaryependymoma may be altered by the extent of disease and surgical resectability. Figure 2. Axial (a) and sagittal (b) T2 images demonstrate hyperintense multifocal intradural masse filling the thecal sac. Pathology: Subsequently, the patient was scheduled for an L5-S1 hemilaminotomy and biopsy was performed by Neurosurgery. Pathohistology showed the L5-S1 mass to be myxopapillaryependymoma. The specimen received consisted of multiple gelatinous translucent grey tissue fragments, measuring in aggregate dimensions 1.5 x 0.5 x 0.1 cm. Histologically, it consisted of fairly small uniform cuboidal tumor cells surrounded by mucinous material collected in microcystic spaces. This mucinous material also collected around hyalinized cores containing blood vessels. The histologic appearance was typical of myxopapillaryependymoma [Figure 4]. Figure 4. Histologic specimen showing a hyalinized vascular core surrounded by mucinous material collected in microcystic spaces and uniform cuboidal tumor cells. Figure 3. Axial (a) and sagittal (b) T1 post-contrast images show that the masses exhibit intense gadolinium enhancement. Imaging & Management Background • Ependymomasare intramedullary CNS tumors arising from ependymal cells that line the cerebral ventricles and the central canal of the spinal canal. They constitute less than 4% of all primary CNS tumors in adults and tend to form centrally within the spinal cord. • Subtypes of Ependymomas: The World Health Organization (WHO) classifies ependymomas into the following four categories: • subependymomas (WHO grade 1) • myxopapillaryependymomas (WHO grade 1) • ependymomas (WHO grade 2) • anaplasticependymomas (WHO grade 3) Among these types, myxopapillaryependymoma is characterized as a slow growing tumor with preferential manifestation in young adults. Myxopapillaryependymoma is located exclusively in the conusmedullaris or the caudaequina or film terminale region, and is rarely found as a multi-focal type. • Pathology: In most myxopapillaryependymomas, the histological examination reveals low mitotic activity that is associated with a low MIB-1 labeling index (LI)2. The prognosis is generally favorable 3. However, late recurrence, distant metastases and subarachnoid disseminations have been reported 4-6. • Clinical Presentation: Patients may initially present with nonspecific local pain in their lower back, leg, or sacral area lasting several months in duration and may later develop further symptoms such as sensory disorders, motor weakness, truncal ataxia and walking disorder, or respiratory distress 9-10. • Imaging: On MRI, ependymomas often appear as symmetric expansions of the spinal cord that are hypointense or isotense compared to normal cord on T1-weighted images with variable signal on T2-weighted images. Postcontrast T1 weighted imaging can improve definition of tumor margins, identify additional tumor cysts, and aid in interpretation of spinal cord after surgical manipulation. Imaging Modality: Magnetic resonance imaging can non-invasively identify myelopathies and is the imaging modality of choice to investigate spinal cord lesions. Distinguishing ependymomas from other CNS neoplasms is important because these tumors can often be completely resected without need for further treatment 23-24. Differential Diagnosis: Other diagnoses that should be included in the differential include hemangioblastoma, paragangliomas, neural cysts, meningioma, and metastases 24. Imaging of the entire neuroaxis should be done to rule out other pathology 25-26. Incidence: The multifocal presentation of myxopapillaryependymoma is rare. Hanbali et al. reported that 2 out of 26 patients with myxopapillaryependymomas had multifocal tumors27. Treatment: Most ependymomas have well-defined margins and are encased by a thin pseudocapsule that separates it from normal cord, and total resection can be safely completed23. Involvement of the caudaequina or filumterminale, which may occur in the multifocal type, makes total resection difficult. In the series reported by Hanbali et al.,one case of the multifocal type had tumor recurrence after surgery27. Sonneland et al, in their analysis of 77 cases with myxopapillaryependymoma, reported that total removal had a recurrence rate of 10%, whereas those that were removed either piecemeal or subtotally had recurrence rates of 19% 3. It is important to closely monitor patients with subtotal surgical removal of tumor. Follow-Up Care: In the present case, cranio-spinal radiation therapy was carried out after surgery because the patient had a subtotal surgical removal. The postoperative course of the present case was uneventful during follow-up. The patient had no tumor recurrence in the brain, spinal cord or the caudaequina. Chemotherapy was not added because there is little data available on the benefit of chemotherapy for spinal cord ependymomas. It will be necessary to continue following this patient very carefully because of subtotal resection of tumor. Prognosis: Although the radiologic multifocal presentation suggested a more aggressive disease, this tumor was slow growing with low mitotic activity, similar to most myxopapillaryependymomas. Usually, the histological character of the ependymoma does not seem to affect long-term prognosis. Size and site of tumor can impact long-term prognosis, and preoperative neurological status is most suggestive of the functional recovery after surgery. The best long term functional recovery occurs with surgical tumor removal. References (1). Louis DN, Ohgaki H, Wiestler OD, et al. The 2007 WHO classification of tumours of the central nervous system. Acta Neuropathol. 2007;114:97–109. (2). Prayson RA. Myxopapillary ependymomas: a clinicopathologic study of 14 cases including MIB-1 and p53 immunoreactivity. Mod Pathol. 1997;10:304–310. (3). Sonneland PR, Scheithauer BW, Onofrio BM. Myxopapillary ependymoma: a clinicopathologic and immunocytochemical study of 77 cases. Cancer. 1985;56:883–893. (4) Guidetti B, Mercuri S, Vagnozzi R. Long-term results of the surgical treatment of 129 intramedullary spinal gliomas. J Neurosurg. 1981;54:323–330. (5). Cooper PR. Outcome after operative treatment of intramedullary spinal cord tumors in adults: intermediate and long-term results in 51 patients. Neurosurgery. 1989;25:855–859. (6) Gomez DR, Missett BT, Wara WM, et al. High failure rate in spinal ependymomas with long-term follow-up. Neuro Oncol. 2005;7:254–259. (7) Findlay, G. Intrinsic spinal cord tumors. In: Handbook of Clinical Neurology, Vol 24: Neuro-Oncology Part II, Vecht, CJ (Ed), Elsevier Science, Amsterdam 1997. p.497. (8) Gilbert, Mark. Roberta Ruda. Riccardo Soffietti. Ependymomas in Adults. Curr Neurol. Neurosci Rep (2010) 10:240–247, Published online: 24 March 2010 (9) Kaner T, Sasani M, Oktenoglu T, Solmaz B, Sarloglu AC, Ozer AF. Clinical analysis of 21cases of spinal cord ependymoma: positive clinical results of gross total resection. J Korean Neurosurg Soc. 2010 Feb;47(2):102-6. (10) Oztekin, Ozgur; Ozan, Ebru; Unal, Gokhan; Adibelli, Zehra Hilal. An unusual presentation of myxopapillary ependymoma with faecal incontinence and literature review. European Journal of Radiology Extra, Vol. 71, 3, 2009, p. e113-115 (11) Mridha, A. R.; Sharma, M. C.; Sarkar, C. et al. Myxopapillary ependymoma of lumbosacral region with metastasis to both cerebellopontine angles: report of a rare case. Child's Nervous System, Vol. 23, 10, 2007, pp. 1209 – 1213 (12) Verstegen MJ, Bosch DA, Troost D. Treatment of ependymomas: Clinical and non-clinical factors influencing prognosis: a review. Br J Neurosurg. 1997; 11: 542-553. (13) Donahue B, Steinfeld A. Intracranial ependymoma in the adult patient: successful treatment with surgery and radiotherapy. J Neurooncol. 1998; 37: 131-133. (14) Shaw EG, Evans RG, Scheithauer BW, Ilstrup DM, Earle JD. Postoperative radiotherapy of intracranial ependymoma in pediatric and adult patients. Int J Radiat Oncol Biol Phys. 1987; 13:1457-1462. (15) Kucia EJ, Maughan PH, Kakarla UK et al.. Surgical technique and outcomes in the treatment of spinal cord ependymomas: part II: myxopapillary ependymoma. Neurosurgery.2011; 68: 90-94; 94. (16) Abdel-Wahab M, Etuk B, Palermo J et al. Spinal cord gliomas: A multi-institutional retrospective analysis. Int J Radiat Oncol Biol Phys. 2006;64(4) (17)Sonneland PR, Scheithauer BW, Onofrio BM. Myxopapillary ependymoma. A clinicopathologic and immunocytochemical study of 77 cases. Cancer. 1985;56(4):883. 18) Wippold F, Smirniotopoulos J, Moran C et al. MR Imaging of Myxopapillary Ependymoma: Findings and Value to Determine Extent of Tumor and its relation to intraspinal structures. American Roentgen Ray Society, 1995. (19) Andoh H, Kawaguchi Y, Seki S et al. Multi-focal Myxopapillary Ependymoma in the Lumbar and Sacral Regions Requiring Cranio-spinal Radiation Therapy: A Case Report. Asian Spine J. 2011 Mar;5(1):68-72. (20) Guidetti B, Mercuri S, Vagnozzi R. Long-term results of the surgical treatment of 129 intramedullary spinal gliomas. J Neurosurg. 1981;54:323–330. (21) Cooper PR. Outcome after operative treatment of intramedullary spinal cord tumors in adults: intermediate and long-term results in 51 patients. Neurosurgery. 1989;25:855–859. (22).Gomez DR, Missett BT, Wara WM, et al. High failure rate in spinal ependymomas with long-term follow-up. Neuro Oncol. 2005;7:254–259. (23) Aghayev K, Vrionis F, Chamberlain MC. Adult intradural primary spinal cord tumors. J Natl Compr Canc Netw. 2011 Apr;9(4):434-47. (24) Do-Dai, Daniel D., Brooks, Michael K.; Goldkamp, Allison; Erbay, Sami; Bhadelia, Rafeeque A.. Magnetic Resonance Imaging of Intramedullary Spinal Cord Lesions: A Pictorial Review. Current Problems in Diagnostic Radiology, Volume 39, issue 4 (July - August, 2010), p. 160-185 (25) Wippold F, Smirniotopoulos J, Moran C et al. MR Imaging of Myxopapillary Ependymoma: Findings and Value to Determine Extent of Tumor and its relation to intraspinal structures. American Roentgen Ray Society, 1995. (26) Chamberlain MC, Sandy AD, Press GA. Spinal cord tumors: gadolinium-DTPA-enhanced MR imaging. Neuroradiology. 1991; 22: 231-45. (27) Hanbali F, Fourney DR, Marmor E, et al. Spinal cord ependymoma: radical surgical resection and outcome. Neurosurgery. 2002;51:1162–1172. (28) Akyurek S, Chang EL, Yu TK, et al. Spinal myxopapillary ependymoma outcomes in patients treated with surgery and radiotherapy at M.D. Anderson Cancer Center. J Neurooncol. 2006;80:177–183. (29). Fakhrai N, Neophytou P, Dieckmann K, et al. Recurrent spinal ependymoma showing partial remission under Imatimib. Acta Neurochir (Wien) 2004;146:1255–1258.