Download
1 / 20
200 likes | 556 Vues
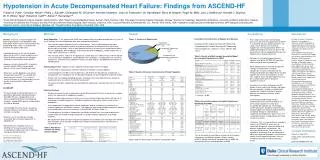
Admission BNP and In-Hospital Mortality in ADHF . Levels of BNP and NT-proBNP have been shown to be elevated in patients with left ventricular (LV) dysfunction and correlate with the New York Heart Association functional class Clinical investigations of natriuretic peptides have focused on the diagnostic usefulness for heart failure (HF) and LV dysfunction and their prognostic usefulness in chronic HF, acute coronary syndromes, stable coronary artery disease, other medical conditions, and comm9446

E N D
1. Admission B-Type Natriuretic Peptide Levels and In-Hospital Mortality in Acute Decompensated Heart Failure
2. An elevated admission BNP level is a significant independent predictor of in-hospital mortality in acute HF with either reduced or preserved LVEF independent of other clinical and laboratory variables.
In light of the demonstration of incremental prognostic information, the BNP assay should be considered for inclusion as part of the standard assessment of all patients presenting with acute decompensated HF.
Further research will be necessary to determine if patients with higher admission BNP will benefit from more intensive monitoring and aggressive treatment strategies.An elevated admission BNP level is a significant independent predictor of in-hospital mortality in acute HF with either reduced or preserved LVEF independent of other clinical and laboratory variables.
In light of the demonstration of incremental prognostic information, the BNP assay should be considered for inclusion as part of the standard assessment of all patients presenting with acute decompensated HF.
Further research will be necessary to determine if patients with higher admission BNP will benefit from more intensive monitoring and aggressive treatment strategies.
3. The ADHERE Registry
4. Initial BNP Levels in ADHERE Time Period: Q2 2003 � Q4 2004
191 out of 229 ADHERE hospitals (176 BNP only, 15 BNP and pro-BNP, 14 pro-BNP only, 24 none)
First BNP result, within 24 hours of admission
Results as documented in medical record
48,629 (63%) out of 77,467 pt episodes had BNP assessment
Analysis by BNP quartiles, continuous, and log transformed BNP
5. Admission BNP and In-Hospital Mortality in ADHF Distribution of BNP Values From April 2003 through December 2004 there were 48,629 eligible acute HF hospitalization episodes in the ADHERE Registry with documented BNP level and LVEF (LVEF > 40%, N = 18,164; LVEF < 40%, N = 19,544). BNP levels were < 100 in only 3.3% of the total cohort hospitalized with a primary discharge diagnosis of HF.
From April 2003 through December 2004 there were 48,629 eligible acute HF hospitalization episodes in the ADHERE Registry with documented BNP level and LVEF (LVEF > 40%, N = 18,164; LVEF < 40%, N = 19,544). BNP levels were < 100 in only 3.3% of the total cohort hospitalized with a primary discharge diagnosis of HF.
6. Admission BNP and In-Hospital Mortality in ADHF BNP Quartiles
Quartile I: < 430 pg/mL
Quartile II: 430 � 839 pg/mL
Quartile III: 840 � 1729 pg/mL
Quartile IV: > 1730 pg/mL Charts for hospitalization episodes from April 2003 through December 2004 were included if BNP levels on admission were recorded for the patient. Patients with quantitative LV function documented during or prior to index hospitalization were included in the subgroup analysis of reduced vs. preserved LV function.
For this analysis we divided patients by BMI quartiles where:
Quartile I: < 430 pg/mL
Quartile II: 430 � 839 pg/mL
Quartile III: 840 � 1729 pg/mL
Quartile IV: > 1730 pg/mL
In-hospital mortality for the entire cohort and for patients with preserved (LVEF > 40%) vs. reduced (LVEF < 40%) systolic function was assessed according to BNP quartile.Charts for hospitalization episodes from April 2003 through December 2004 were included if BNP levels on admission were recorded for the patient. Patients with quantitative LV function documented during or prior to index hospitalization were included in the subgroup analysis of reduced vs. preserved LV function.
For this analysis we divided patients by BMI quartiles where:
Quartile I: < 430 pg/mL
Quartile II: 430 � 839 pg/mL
Quartile III: 840 � 1729 pg/mL
Quartile IV: > 1730 pg/mL
In-hospital mortality for the entire cohort and for patients with preserved (LVEF > 40%) vs. reduced (LVEF < 40%) systolic function was assessed according to BNP quartile.
7. Patient Characteristics by Quartiles of BNP Levels in the ADHERE Registry
8. Patient Characteristics by Quartiles of BNP Levels in the ADHERE Registry
9. Patient IV Treatments by Quartiles of BNP Levels in the ADHERE Registry
10. Admission BNP and In-Hospital Mortality in ADHF In-hospital Medications More than twice as many patients in QIV vs. QI were treated with nesiritide. The same relationship held for those treated with inotropes. Most patients received IV diuretic (90% - 94%).
The median time to first diuretic was essentially the same for all groups (2.4 � 2.6 hrs).
More than twice as many patients in QIV vs. QI were treated with nesiritide. The same relationship held for those treated with inotropes. Most patients received IV diuretic (90% - 94%).
The median time to first diuretic was essentially the same for all groups (2.4 � 2.6 hrs).
11. In-Hospital Mortality Risk by Initial BNP Levels in the ADHERE Registry
12. In-Hospital Mortality Risk by Initial BNP Levels in the ADHERE Registry
13. In-Hospital Mortality Risk by Initial BNP Levels Reduced vs. Preserved Systolic Function HF
16. TOTAL HOSPITAL LENGTH OF STAY STRATIFIED BY BNP QUARTILE
17. Patient Outcomes by Quartiles of BNP Levels in the ADHERE Registry
18. Admission BNP and In-Hospital Mortality in ADHF Study Limitations Data collected from chart review which is dependent on the accuracy and completeness of documentation and abstraction
This �real world� study used results of various commercially available BNP assays vs. results from single central core laboratory
Individual hospitalization episodes vs. individual unique patients
Each hospitalization represents unique opportunity to either survive or not survive. Data are collected by medical chart review and are thus dependent upon the accuracy and completeness of documentation and abstraction.
BNP levels were analyzed at individual hospitals using the various commercially available assays, rather than a single central laboratory.
ADHERE� accumulates data on individual hospitalizations, not on individual patients, however, each hospitalization episode represents a unique opportunity to either survive or not-survive.
Data are collected by medical chart review and are thus dependent upon the accuracy and completeness of documentation and abstraction.
BNP levels were analyzed at individual hospitals using the various commercially available assays, rather than a single central laboratory.
ADHERE� accumulates data on individual hospitalizations, not on individual patients, however, each hospitalization episode represents a unique opportunity to either survive or not-survive.
19. Admission BNP and In-HospitalMortality in ADHF Elevated admission BNP is a significant predictor of in-hospital mortality in ADHF, independent of other risk factors
BNP is predictive of mortality in both patients with reduced and those with preserved LVEF
Further research necessary to determine whether pts with higher admission BNP would benefit from more intensive monitoring and/or aggressive treatment strategies An elevated admission BNP level is a significant independent predictor of in-hospital mortality in acute HF with either reduced or preserved LVEF independent of other clinical and laboratory variables.
In light of the demonstration of incremental prognostic information, the BNP assay should be considered for inclusion as part of the standard assessment of all patients presenting with acute decompensated HF.
Further research will be necessary to determine if patients with higher admission BNP will benefit from more intensive monitoring and aggressive treatment strategies.An elevated admission BNP level is a significant independent predictor of in-hospital mortality in acute HF with either reduced or preserved LVEF independent of other clinical and laboratory variables.
In light of the demonstration of incremental prognostic information, the BNP assay should be considered for inclusion as part of the standard assessment of all patients presenting with acute decompensated HF.
Further research will be necessary to determine if patients with higher admission BNP will benefit from more intensive monitoring and aggressive treatment strategies.
20. The ADHERE Scientific Advisory Committee and Investigators