Download
1 / 21
630 likes | 1.61k Vues
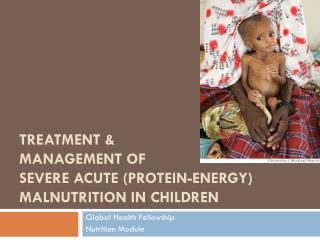
Community Management of Acute Malnutrition (CMAM) (an overview). National Nutrition Advocacy Meeting 15 July 2012. Anirudra Sharma Nutrition Specialist UNICEF. Status of wasting (by eco-regions). Overview of Community based Management National Scale Up Plan. 2012 - 2017.

E N D
Community Management of Acute Malnutrition (CMAM) (an overview) National Nutrition Advocacy Meeting 15 July 2012 Anirudra Sharma Nutrition Specialist UNICEF
Status of wasting (by eco-regions) • Overview of Community based Management National Scale Up Plan 2012 - 2017 Source: NDHS 2011
CMAM Pilot Districts FAR-WESTERN REGION HUMLA MID-WESTERN REGION • Darchula • Simikot DARCHULA BAJHANG MUGU BAITADI • Chainpur • Martadi • Gamgadi • Baitadi BAJURA • Dadeldhura • Jumla DADEL- • Dipayal KALIKOT JUMLA ACHHAM DHURA WESTERN REGION DOTI DOLPA • Magalsen • Manma MUSTANG • Dailekh • Dunai KANCHAN- JAJARKOT PUR DAILEKH • Jomosom • Mahendranagar • Jajarkot RUKUM KAILALI MANANG • Dhangadi • Birendranagar • Jumlikhalanda CENTRAL REGION MYAGDI • Chame SURKHET BARDIYA ROLPA BAGLUNG • Beni SALYAN • Salyan GORKHA KASKI • Gularia • Liwang • Kusma LAMJUNG • Baglung • Pokhara EASTERN REGION PARBAT RASUWA • Besisahar • Gorkha BANKE PYUTHAN GULMI • Syangja • Dhunche • Nepalgunj • Pyuthan • Tamghas TANAHU DHADING DANG SYANGJA SINDHU- • Sandhikharka • Damauli NUWAKOT PALCHOK • Ghorahi ARGHAKHACHI • Tansen • Bidur DOLAKHA PALPA • Dhadingbesi • Chautara KTM KAPILBASTU NAWALPARASI SOLUK- B Legend • Taulihawa RUPANDEHI • Bharatpur • Charikot HUMBU SANKHUWA- P • Sidharthanagar • Parasi • Hetauda TAPLEJUNG A Patan KAVRE H SABA CHITWAN • Ramechhap • Salleri H C E MAKAWANPUR • Dhulikhel OKHAL- • Khandbari • Taplejung M A DHUNGA R PARSA • Sindhulimadi • Okhaldhunga • Diktel • Bhojpur • Terhathum SINDHULI KHOTANG R A BARA RAUTA- TERHA- H BHOJ- T E • Birgunj HAT THUM H PUR C • Kalaiya • Dhankuta A P UDAYAPUR SARLAHI MAHO- • Gaur DHANUSA DHANKUTA • Phidim TARI • Malangwa • Ilam ILAM • Gaighat SIRAHA Jaleshwor • Janakpur • Siraha • Ineruwa MORANG SUNSARI JHAPA SAPTARI • Rajbiraj • Chandragadi CMAM Pilot • Biratnagar
Situation of Emergencies in 2007/08 in Nepal Droughts in hills and mountains Floods in terai regions Severe food insecurity in many hills and mountain districts A traditional seasonal out-migration Disease epidemics – diarrhoea/cholera Global Acute malnutrition was in critical threshold - 13% nationwide and <15% in many districts Impact of the ten-year lasting armed conflict with high migration, displacement – disruption of basic social services, dysfunctional authorities, absenteeism of human resources Poor socio economic status Concentrated epidemic of HIV and AIDS Increased 3F (financial, food and fuel) crisis
As per the Baseline Survey, the Status of Under Five Wasting in Five Pilot Districts was…………….
Severity of Nutrition Crisis ( WHO Benchmarks) Emergency Threshold Source: WHO, Management of Malnutrition in Major Emergencies, 2000
Steps towards CMAM Pilot Dec 2007: Conducted feasibility study October 2007: Organized orientation workshop for potential partners March 2008: Organized child health sub-committee meeting on protocol & implementation framework; and finalized national guideline and treatment protocol June 2008: MoHP approved emergency nutrition policy, including CMAM piloting; and conducted CMAM baseline survey January 2009: Organized national pilot planning meeting, organized Master TOT; and Started implementation in three districts Sept. 2010: Implemented in next two districts 2010/2011: CMAM is Recommended for national scale up from SUN initiative, health sector nutrition evidence review and formative evaluation 2012: DHS/MoHP decided for national scaling up CMAM in new 6 districts; and pipeline in 9 additional districts
Goal of CMAM Create increased access to treatment for (severe) acute malnutrition by bringing appropriate nutrition services (including awareness raising, outreach and counseling for prevention) nearer to the community The Objective of CMAM pilot in Nepal To evaluate the feasibility of the CMAM approach in different districts and different agro-ecological zones in Nepal. Following the monitoring and evaluation of the programme, recommendations will be made to the MoHP as regards treatment of acute malnutrition and the potential scale-up of the CMAM approach to most of the districts in the country.
Principles and Components of CMAM • Identification of key individuals in community for activities • Community case finding • Promote understanding of programme and who is eligible • Dialogue on barriers to uptake • Case referral • Case follow up • Counselling • Defaulter follow up Principles: • Maximum access and coverage • Timeliness • Appropriate medical and nutrition care • Care for as long as needed Components:
Classification for Acute Malnutrition(new classification by WHO) *Complications: severe oedema, marasmic-kwashiorkor, anorexia, intractable vomiting, convulsions, lethargic, lower respiratory track infection, high fever, severe dehydration, severe anaemia, hypoglycaemia, hypothermia
CMAM Stakeholders in Nepal National Lead: Child Health Division of DoHS/MoHP Implementing Agencies: • District Public/Health Offices including local health system/structures • Local NGOs • Local Governance Institutions (DDC and VDCs) Support agency: • UNICEF • EU • DFID • ACF
Why CMAM National Scale Up is Needed • Stagnant Status of Acute Malnutrition since last decade • Approx. 385,000 under five children are GAM (91,000 SAM) at a point of time and it could be 2 times or more case load throughout a year i.e. 770,000 Moderately Acute Malnourished 182,000 Severely Acute Malnourished per year-more than WHO defined crisis threshold • WHO estimates have shown that mortality among children with severe acute malnutrition (SAM) is 5 to 20 times higher compared to well-nourished children • Aggravating factors and immediate determinants such as infections, insufficient food intake, different types of disasters for GAM are widely prevalent • Approx. 2/3rd of total districts (50 districts) cross the crisis threshold throughout the country • CMAM is recommended for national scale up by health sector nutrition evidence review and therefore, it is endorsed in MSNP for national scale up to address the issues of SAM
5. Strengthen and improve WASH facilities in OTPs/ SCs Hygiene promotion CMAM Scaling Up Modality 3. In-patient treatment programme (SCs/NRH) 2. Out-patient treatment programme (OTPs) 4. Programmes to address MAM (capacity building and Counselling of family and communities on IYCF and care, health, ECD, and WASH) Community outreach/social mobilization/ Screening
CMAM in Nepal FAR-WESTERN REGION HUMLA MID-WESTERN REGION • Darchula • Simikot DARCHULA BAJHANG MUGU BAITADI • Chainpur • Martadi • Gamgadi • Baitadi BAJURA • Dadeldhura • Jumla DADEL- • Dipayal KALI KOT JUMLA ACHHAM DHURA WESTERN REGION DOTI DOLPA • Magalsen • Manma MUSTANG • Dailekh • Dunai KANCHAN- JAJARKOT PUR DAILEKH • Jomosom • Mahendranagar • Jajarkot RUKUM KAILALI MANANG • Dhangadi • Birendranagar • Jumlikhalanda CENTRAL REGION MYAGDI • Chame SURKHET BARDIYA ROLPA BAGLUNG • Beni SALYAN • Salyan GORKHA KASKI • Gularia • Liwang • Kusma LAMJUNG • Baglung • Pokhara EASTERN REGION PARBAT RASUWA • Besisahar • Gorkha BANKE PYUTHAN GULMI • Syangja • Dhunche • Nepalgunj • Pyuthan • Tamghas TANAHU DHADING DANG SYANGJA SINDHU- • Sandhikharka • Damauli NUWAKOT PALCHOK • Ghorahi ARGHAKHACHI • Tansen • Bidur DOLAKHA PALPA • Dhadingbesi • Chautara KTM KAPILBASTU NAWALPARASI SOLUK- B Legend • Taulihawa RUPANDEHI • Bharatpur • Charikot HUMBU SANKHUWA- P • Sidharthanagar • Parasi • Hetauda TAPLEJUNG A Patan KAVRE H SABA CHITWAN • Ramechhap • Salleri H C E MAKAWANPUR • Dhulikhel OKHAL- • Khandbari • Taplejung M A DHUNGA R PARSA • Sindhulimadi • Okhaldhunga • Diktel • Bhojpur • Terhathum SINDHULI KHOTANG R A BARA RAUTA- TERHA- H BHOJ- T E • Birgunj HAT THUM H PUR C • Kalaiya • Dhankuta A P UDAYAPUR SARLAHI MAHO- • Gaur DHANUSA DHANKUTA • Phidim TARI New CMAM districts, 2012 • Malangwa • Ilam ILAM CMAM pilot districts • Gaighat SIRAHA Jaleshwor • Janakpur • Siraha • Ineruwa MORANG SUNSARI JHAPA SAPTARI • Rajbiraj • Chandragadi Districts in the pipeline for CMAM implementation, 2012/13 • Biratnagar
CMAM Scaleup Plan (proposed)(Considering >10% GAM Threshold)
Challenges • Considering CMAM intervention as development agenda • RUTF procurement and supply and local production • Addressing the issues of MAM – assessment of economic feasibility, sustainability and acceptance of the food based nutrition approach as compared to alternative approaches (strengthened IYCF counseling, ECCD, WASH) and voucher scheme or cash transfer • The aggravating factors for wasting such as - monsoon floods, diarrhea epidemic and current social strata and vulnerabilities • Resources for national scale up – the major challenges – Resources?? Donors support??
Way Forward • Incorporated in GoN regular AWPB for CMAM scale-up and advocacy with EDPs for sustained financing • Establish and strengthen adequate coordination among service providers • Build sufficient capacity of national duty bearers/only few organizations are working in emergency nutrition sectors • Strengthening community outreach • HR management and development • Regular capacity building of health workers and volunteers • Quality monitoring and supervision • Programme integration