Download
1 / 52
520 likes | 721 Vues
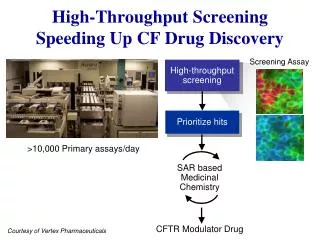
Implementation and Dissemination of Alcohol Screening and Follow-up Using Tools in CPRS/VistA. Katharine Bradley, MD Dan Kivlahan, PhD Carol Achtmeyer, MN, ARNP Emily Williams, MPH Gwen Lapham, MSW Supported by NW HSRD; RWJ Foundation; SUD QUERI; CESATE; VA Puget Sound. Overview.

E N D
Implementation and Dissemination of Alcohol Screening and Follow-up Using Tools in CPRS/VistA Katharine Bradley, MD Dan Kivlahan, PhD Carol Achtmeyer, MN, ARNP Emily Williams, MPH Gwen Lapham, MSW Supported by NW HSRD; RWJ Foundation; SUD QUERI; CESATE; VA Puget Sound
Overview Implementation of 2Two CPRS Clinical Reminders Alcohol screening Follow-up positive alcohol screens
Outline Background alcohol misuse VistA/CPRS components and approaches used Clinical reminders Health factors Mental health package Clinical informatics expert Case Study #1 - Screening Local National Case Study #2 - Brief alcohol counseling Local Regional National Next steps
Background Alcohol misuse is common & large health burden Evidence supports preventive focus Brief alcohol counseling interventions effective Target population: patients with risky drinking Advice and feedback decrease drinking 3rd highest US Prevention Priority-Solberg 2008 Limited implementation of brief alcohol counseling
Alcohol Screening in VA Prior to 2003 Original performance measure (PM) PM required any standardized screen Almost all used CAGE Identifieslifetime alcohol use disorders Does not indicate if patients drink Not the target population for brief alcohol counseling Background
Incremental Implementation 2000 AUDIT-C clinical reminder (CR) - 1 site 2001 Development CR for Follow-up – 1 site 2002 Pilot Study of Follow-up CR – 1 site 2003 New screening Performance Measure 2003 National screening CR: AUDIT-C 2004 Adoption of Follow-up CR by large VA 2007 Screening PM modified 2007 National PM for Follow-up Positive AUDIT-Cs 2008 National Follow-up CR disseminated
Key Concepts Required for HIT implementation • System and HIT readiness (at same time) • Linkage between researchers/HIT developers and informatics, clinical, and QI leaders • Clinical informatics expert on research team • Creative financing – not on project timeline • Greenhalgh model (2004) has been helpful understanding success and failures
CPRS/VistA Tools for Implementation Research Intro to Clinical Reminders (CRs) CPRS Clinical Reminders can … Alert providers to clinical care due Educate providers Provide decision support Document care Be shared between facilities Provide data for performance monitoring Activated for specific providers CR reports can monitor in real time
Intro to CPRS Clinical Reminders Provider Opens Progress Note Provider MAY open Reminders Window
Intro to CPRS Clinical Reminders Progress Note Provider MAY choose to address follow-up for a positive alcohol misuse screen
Intro to CPRS Clinical Reminders Clicking on Reminders Button and CR name brings up reminder dialog
Intro to CPRS Clinical Reminders Decision Support Health Factors are sent to VistA when boxes are clicked
Health factors Can be attached to specific actions in CRs and used to monitor CR activity Are not standardized, so vary across sites and over time Stored locally in VistA, in some regional data warehouses and CDW Mental Health Assistant (MHA) Standardized assessment instruments Scored automatically Standardized data Data stored in local VistA, eventually Pittsburg CPRS/VistA Tools for Implementation Research
CPRS/VistA Tools for Implementation Research CPRS GUI Clinical Reminders VistA Files Prog.Notes Health Factors MH Package Pharmacy Labs
Clinical Informatics Expert Prescribing clinician Familiar with basic VistA and CPRS functions Knew local programmers Entrepreneurial Initial role: project-oriented Evolved to multiple roles Builds clinical reminders, order sets etc. Monitoring developments in CPRS Networking within informatics community Identify/develop data sources Obtaining VistA data
Clinical Informatics Expert Staying on the “cutting edge” Attend annual VeHU conferences, online trainings Weekly calls on CPRS or Clinical Reminders American Informatics Medical Association (AMIA) Review research on VA CPRS Maintaining access to CPRS Service to local facility Beta test new CPRS software Creative Financing: non-VA funding, Clinical COE (CESATE); and QUERI core funds
Case Study #1 Screening Clinical Reminder Local (2000-2007) National (2004-2008) Case Study #1
AUDIT-C 3-item screen (0-4 each): sum to 0-12 Identifies the target population for brief alcohol counseling Described/validated in VA outpatients 1998 Case Study #1 - Alcohol Screening
AUDIT-Cinto the MHA Papers shared with Office of Mental Health 2 AUDIT-Cs added to MHA (self-scoring) Technical problems with MHA AUDIT-C Could not be corrected locally Case Study #1 - Alcohol Screening
Local Implementation of AUDIT-C ~ 2000 Local decision to use AUDIT-C Based on review of evidence Request for MH programmers to fix MHA AUDIT-C Meanwhile local AUDIT-C CR built: not self-scoring AUDIT-C in MHA for years with no use Case Study #1 - Alcohol Screening
National Implementation of AUDIT-C 2003 Office of Quality and Performance (OQP) sought guidance for next steps Among VA patients who had 4+ drinks/day 66% felt they needed services for drinking Only 17% reported they got needed services OQP educated: need to screen for risky drinking Case Study #1 - Alcohol Screening
Invitation to give key national presentations Quality Management Information Conferences (2) Performance Measures Work Group (PMWG) PMWG decides to require AUDIT-C in FY 2004 National demand for new informatics tools for self scoring AUDIT-C Case Study #1 - Alcohol Screening
OQP convened call develop AUDIT-C clinical reminder Content experts (researchers) Research clinical informatics expert National CR expert Associate Chief Consultant for MH Informatics OQP leader in charge of PM Barrier: self scoring AUDIT-C still needed fixing Case Study #1 - Alcohol Screening
Clinical informatics expert Knew problems with MHA AUDIT-C’s Boundary spanner Barrier: AUDIT-C in MH package lacked response options for nondrinkers Led to 2 step clinical reminder Identify drinkers Administer AUDIT-C National expert built AUDIT-C CR CR made available nationally Case Study #1 - Alcohol Screening
Passive diffusion AUDIT-C in MHA used 1.4 million times in 2004 Lack of “buy-in” End-users not familiar with AUDIT-C New paradigm: preventive counseling FAQ posted by OQP educated the field SHEP survey used to evaluate Problems in quality: nondrinkers and under reporting Revised PM in 2007 Case Study #1 - Alcohol Screening
Facilitators System readiness Collaboration: researchers, informatics & clinical leaders HIT tool is available when system is ready Characteristics of the innovation diffusion Evaluation and feedback Comparison of survey & clinical screening Resulted in revised Performance Measure Case Study #1 - Alcohol Screening
Barriers HIT not ready when PM announced Decision made to use 2 step screening: non-standard assessment of drinking Initially unprepared for educational need Problems with face validity of AUDIT-C Lack of provider buy-in Lack of awareness of the importance of how screening is completed (verbatim; private; non-judgmental) Case Study #1 - Alcohol Screening
Follow-up Clinical Reminder Local (2001-2005) Regional (2004-2006) National (2008) Case Study #2
Local Pilot Follow-up Clinical Reminder Version 1 (2001) Original idea Simple feedback of screening results to providers; relied on CPRS programmers CPRS expert hired to help not feasible CPRS expert clinical reminders Version 1 clinical reminder content based on trials Assumed provider would do full assessment Focus groups Case Study #2A – Follow-up Clinical Reminder
Follow-up Clinical Reminder Version 1 (2001) Modifications after focus group feedback Simpler algorithm and help text Only advice initially required Escape option: “Will address at next visit” Optional Assessment: diagnostic criteria, labs, blood pressure, readiness to change Intervention: patients goal, referral, etc. Case Study #2A – Follow-up Clinical Reminder
Case Study #2A – Follow-up Clinical Reminder Provider Education: recommended drinking limits Provider Education: Components of BI
Case Study #2A – Follow-up Clinical Reminder • Provides Decision Support • Risk Stratify: Assess prior treatment and whether drinking above limits • Advise:required to “turn off” clinical reminders • Optional: Document giving feedback on medical problems linked to alcohol use, further assessment, or referral
Case Study #2A – Follow-up Clinical Reminder Facilitates documentation Each action clicked is documented in progress note Turns off clinical reminder if advice documented Click “Finish” button
Local Pilot Follow-up Clinical Reminder (2003-2005) Tested locally after revision Primary care providers did not routinely use CRs No specific training: email announcement only Health factors from regional data warehouse Low rates of use: 15% Many noted would address alcohol at another visit Case Study #2A – Follow-up Clinical Reminder
Case Study #2A – Follow-up Clinical Reminder Local Pilot (2003-2005) Facilitators • Clinical informatics expert • Identified tools • Built and reiteratively revised clinical reminder • Early linkage with local end-users • 1:1 observation and focus groups key Barriers • VA providers hard to recruit for focus groups • Low system readiness
National implementation of AUDIT-C screening “The field” wanted help with follow-up National CR experts requested follow-up CR One expert Simplified and implemented the CR at 8 sites Shared with other sites Health factors simplified and changed Used CPRS CR Reports to track Submitted IRB application Case Study #2B – Follow-up Clinical Reminder Informal RegionalDissemination
Case Study #2B – Follow-up Clinical ReminderInformal RegionalDissemination % Patients with Positive AUDIT-C whose Provider Completed CR for Brief Alcohol Counseling Bradley Substance Abuse 2007
Case Study #2B – Follow-up Clinical ReminderInformal RegionalDissemination % Patients with Positive AUDIT-C whose Provider Completed CR for Brief Alcohol Counseling
Evaluation CR reports provide no detail on parts of CR used CIE worked to get MHA data out of VistA (VeHU) National fileman expert wrote Fileman query CIE Tested locally, then sent to pilot site Pilot site built locally extracted data ASCII file transferred server to server STATA Health factor data difficult to interpret *CIE=clinical informatics expert Case Study #2B – Follow-up Clinical ReminderInformal RegionalDissemination
Case Study #2B – Follow-up Clinical ReminderInformal RegionalDissemination Facilitators • System readiness • Performance measure for screening created demand for Follow-up CR at some sites • Primary care providers routinely used CR • CIE - Informal informatics networks • Improved/adapted clinical reminder • 2nd Pilot – 8 sites • Allowed us to get data from that site Barriers • Finding MHA data • Health factor data edited; not distinct names
Case Study #2B-C – Follow-up Clinical ReminderImproving the CR for NationalDissemination Quality Improvement before Dissemination • OQP consulted: Follow-up EPRP measures (6/2006) • Collaboration on Follow-up CR (5/2007) • OQP and OMHS • national CR expert CR • But no formative evaluation of CR yet! • How are providers using the CRs? • What needs fixing? • Hasty quality improvement interviews • Creative financing: CESATE
Dissemination Clinical reminder adapted again Further simplified based on interviews Made consistent with performance measure Fall 2007: sites could request CR from Office of Primary Care-Mental Health integration Distributed nationally in CPRS CR patch 6, January 2008 Case Study #2C – Follow-up Clinical ReminderNational Dissemination
Case Study #2C – Follow-up Clinical ReminderNational Dissemination Change Over Time in Rates of Documented Brief Alcohol Counseling * Among Patients with AUDIT-C > 5; p’s < 0.001
Case Study #2C – Follow-up Clinical ReminderNational Dissemination Change Over Time in Rates of Documented Brief Alcohol Counseling * Among Patients with AUDIT-C > 5; p’s < 0.001
Case Study #2C – Follow-up Clinical ReminderNational Dissemination Change Over Time in Rates of Documented Brief Alcohol Counseling * Among Patients with AUDIT-C > 5; p’s < 0.001
Case Study #2C – Follow-up Clinical ReminderNational Dissemination Change Over Time in Rates of Documented Brief Alcohol Counseling * Among Patients with AUDIT-C > 5; p’s < 0.001
Next Steps • Standardize follow-up CR for electronic monitoring • Evaluate quality of brief alcohol counseling • Compare documented advice & patient report • Evaluate changes in drinking after counseling • Validate AUDIT-C as a measure of change • Compare quality across implementation strategies • B Yano’s Primary care survey • Work towards having MHA AUDIT-C • interact with the pharmacy package • inserted into pre-op templates • Chronic management alcohol dependence in CPRS • Patient lists, order sets, and templates
Conclusions Challenges for Implementation • Lack of system readiness • Unanticipated “opportunities” quick fixes • Lack of provider education • Changes in leadership • Research funding not well suited • Clinical informatics expert – keeping expertise while on a research team*
Conclusions Important Facilitators • Strong evidence-base • System readiness • Collaboration between researchers & quality improvement / clinical leaders • Flexible funding … and most of all… • Clinical informatics expert
The End Thank You! Bryan Volpp Roxanne Rusch Lynette Nilan Dale Cannon Alan Finkelstein Katy Lysell Ira Katz Michael Mayo-Smith VA Puget Sound Informatics