Download
1 / 91

E N D
Physical Diagnosis Cyanosis
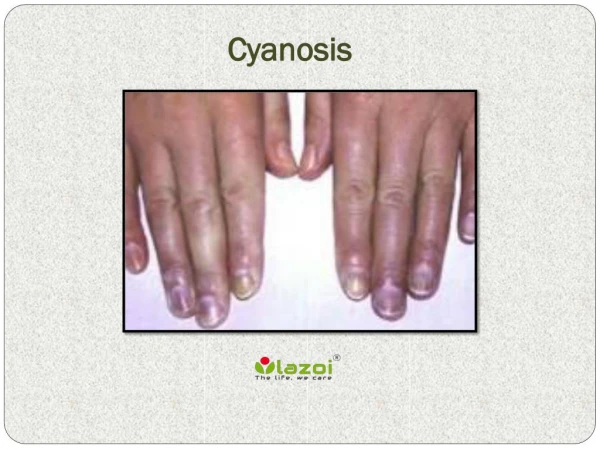
DefinitionCyanosisrefers to a bluish(带蓝色的;带青色的)color of the skin and mucous membranes resulting from an increased quantity of reduced hemoglobin(亚铁血红蛋白;还原血红蛋白), or of hemoglobin derivatives, in the small blood vessels of those areas. It is usually most marked in the lips, nail beds(甲床), ears, and malar(颧骨的;颊的)eminences(隆起).
Definition of cyanosis A bluish color of skin and mucous membranes, especially in lips, nail beds, and malar eminences, caused by increased amount of reduced hemoglobin(Hb) or abnormal Hb derivatives in small blood vessels.
Cyanosis, especially if developed recently, is more commonly detected by a family member than the patient. The florid(鲜红色的;气色好的) skin characteristic of polycythemia vera(真性红细胞增多症) must be distinguished from the true cyanosis discussed here.
A cherry(樱桃)-colored flush(潮红), rather than cyanosis, is caused by COHb(Carboxyhemoglobin 碳氧血红蛋白).
The degree of cyanosis is modified by the color of the cutaneous(皮肤的) pigment and the thickness of the skin, as well as by the state of the cutaneous capillaries.
The accurate clinical detection of the presence and degree of cyanosis is difficult, as proved by oximetric(血氧定量法的)studies.
In some instances, central cyanosis can be detected reliably when the SaO2 has fallen to 85%; in others, particularly in dark-skinned persons, it may not be detected until it has declined to 75%. In the latter case, examination of the mucous membranes in the oral cavity and the conjunctivae(结膜)rather than examination of the skin is more helpful in the detection of cyanosis.
The increase in the quantity of reduced hemoglobin in the mucocutaneous(皮肤粘膜的) vessels that produces cyanosis may be brought about either by an increase in the quantity of venous blood as the result of dilatation of the venules(小静脉) and venous ends of the capillaries or by a reduction in the SaO2 in the capillary blood.
In general, cyanosis becomes apparent when the mean capillary concentration of reduced hemoglobin exceeds 50 g/L (5g/dL). It is the absoluterather than the relativequantity of reduced hemoglobin that is important in producing cyanosis.
Thus, in a patient with severe anemia, the relative amount of reduced hemoglobin in the venous blood may be very large when considered in relation to the total amount of hemoglobin in the blood. However, since the concentration of the latter is markedly reduced, theabsolutequantity of reduced hemoglobin may still be small, and therefore patients with severe anemia and even marked arterial desaturation(稀释)do not display cyanosis.
Conversely, the higher the total hemoglobin content, the greater is the tendency toward cyanosis; thus, patients with marked polycythemia(红细胞增多症)tend to be cyanotic at higher levels of SaO2 than patients with normal hematocrit(红细胞压积) values.
Likewise, local passive congestion, which causes an increase in the total amount of reduced hemoglobin in the vessels in a given area, may cause cyanosis.
Cyanosis also is observed when nonfunctional hemoglobin such as methemoglobin(正铁血红蛋白,高铁血红蛋白)or sulfhemoglobin(硫化血红蛋白) is present in blood.
Mechanisms of Cyanosis Caused by absolute increase of amount of reduced Hb in blood, usually > 5g/dl (capillary) The higher the hemoglobin concentration, The greater tendency toward cyanosis. g/dl Normal Polycythemia Anemia
Clinical Classification & Etiology • True Cyanosis(increased amount of reduced Hb) — Central Type — Peripheral Type — Mixed Type • Cyanosis due to abnormal Hb derivatives — Methemoglobinemia(高铁血红蛋白血症) — Sulfhemoglobinemia(硫化血红蛋白血症)
Cyanosis may be subdivided into central and peripheral types. In the centraltype, the SaO2 is reduced or an abnormal hemoglobin derivative is present, and the mucous membranes and skin are both affected.
Peripheralcyanosis is due to a slowing of blood flow and abnormally great extraction of O2 from normally saturated arterial blood. It results from vasoconstriction and diminished peripheral blood flow, such as occurs in cold exposure, shock, congestive failure, and peripheral vascular disease.
Often in these conditions the mucous membranes of the oral cavity or those beneath the tongue may be spared. Clinical differentiation between central and peripheral cyanosis may not always be simple, and in conditions such as cardiogenic shock (心源性休克)with pulmonary edema(肺水肿)there may be a mixture of both types.
Central Cyanosis Impaired pulmonary function 1. Airway obstruction 2. Pulmonary diseases 3. Pleural(胸膜的)diseases Right-to-left shunting of blood Tetralogy of Fallot
Peripheral Cyanosis Caused by increased oxygen consumption in peripheral tissue. Vasoconstriction Low cardiac output Exposure to cold air or water Slowing of blood flow Right heart failure
Mixed Cyanosis (Central + Peripheral) Pulmonary Edema Cardiogenic Shock
Central CyanosisDecreased SaO2 results from a marked reduction in the PaO2. This reduction may be brought about by a decline in the FIO2(fraction of inspired oxygen 吸人氧气分数)without sufficient compensatory alveolar(肺泡的) hyperventilation(通气过度,换气过度)to maintain alveolar PO2.
Cyanosis does not occur to a significant degree in an ascent to an altitude of 2500 m (8000 ft) but is marked in a further ascent to 5000 m (16,000 ft). The reason for this difference becomes clear on studying the S shape of the Hb-O2 dissociation curve.
At 2500 m (8000 ft) the FIO2 is about 120 mmHg, the alveolar PO2 is approximately 80 mmHg, and the SaO2 is nearly normal.
However, at 5000 m (16,000 ft) the FIO2 and alveolar PO2 are about 85 and 50 mmHg, respectively, and the SaO2 is only about 75%. This leaves 25% of the hemoglobin in the arterial blood in the reduced form, an amount likely to be associated with cyanosis in the absence of anemia.
Similarly, a mutant hemoglobin with a low affinity for O2 (e.g., Hb Kansas) causes lowered SaO2 and resultant central cyanosis.
Seriously impaired pulmonary function, through perfusion(灌注) of unventilated or poorly ventilated areas of the lung or alveolar hypoventilation, is a common cause of central cyanosis.
This condition may occur acutely, as in extensive pneumonia or pulmonary edema, or chronically with chronic pulmonary diseases (e.g., emphysema 肺气肿). In the last situation, secondary polycythemia(红血球增多症) is generally present, and clubbing(杵状指)of the fingers may occur.
However, in many types of chronic pulmonary disease with fibrosis and obliteration(闭塞)of the capillary vascular bed, cyanosis does not occur because there is relatively little perfusion of underventilated areas.
Another cause of reduced SaO2 is shunting of systemic venous blood into the arterial circuit. Certain forms of congenital heart disease are associated with cyanosis.
Since blood flows from a higher-pressure to a lower-pressure region, for a cardiac defect to result in a right-to-left shunt, it must ordinarily be combined with an obstructive lesion distal to the defect or with elevated pulmonary vascular resistance.
The most common congenital cardiac lesion associated with cyanosis in the adult is the combination of ventricular septal defect and pulmonary outflow tract obstruction (tetralogy of Fallot).
The more severe the obstruction, the greater the degree of right-to-left shunting and resultant cyanosis. In patients with patent ductus arteriosus, pulmonary hypertension, and right-to-left shunt, differential cyanosis results; that is, cyanosis occurs in the lower but not in the upper extremities.
Pulmonary arteriovenous fistulae may be congenital or acquired, solitary or multiple, microscopic or massive. The severity of cyanosis produced by these fistulae depends on their size and number.
They occur with some frequency in hereditary hemorrhagic telangiectasia (毛细管扩张). SaO2 reduction and cyanosis may also occur in some patients with cirrhosis, presumably as a consequence of pulmonary arteriovenous fistulas or portal vein-pulmonary vein anastomose(吻合术).
In patients with cardiac or pulmonary right-to-left shunts, the presence and severity of cyanosis depend on the size of the shunt relative to the systemic flow as well as on the Hb-O2 saturation of the venous blood.
With increased extraction of O2 from the blood by the exercising muscles, the venous blood returning to the right side of the heart is more unsaturated than at rest, and shunting of this blood or its passage through lungs incapable of normal oxygenation intensifies the cyanosis.
Also, since the systemic vascular resistance falls with exercise, the right-to-left shunt is augmented by exercise in patients with congenital heart disease and communications between the two sides of the heart. Secondary polycythemia occurs frequently in patients with arterial O2 unsaturation and contributes to the cyanosis.
Cyanosis can be caused by small amounts of circulating methemoglobin and by even smaller amounts of sulfhemoglobin. Although they are uncommon causes of cyanosis, these abnormal hemoglobin pigments should be sought by spectroscopy(分光镜检查)when cyanosis is not readily explained by malfunction of the circulatory or respiratory systems.
Generally, digital clubbing does not occur with them. The diagnosis of methemoglobinemia can be suspected if the patient's blood remains brown after being mixed in a test tube and exposed to air.
Cyanosis due to abnormal Hb derivatives • Methemoglobinemia — Hereditary: very rare — Acquired: >3g/dl in blood - intake or exposure to some drugs or chemicals, such as sulfa drugs, nitrite salt. “ enterogenic cyanosis ” • Sulfhemoglobinemia — Caused by some drugs or chemicals, — Sulfhemoglobin > 0.5g/dl in blood
Approach to Patients with Cyanosis • Differentiation of central as opposed to peripheral Cyanosis Skin temp. Massage(按摩)or warming Central Warm No change Peripheral Cool Cyanosis fades
Probably the most common cause of peripheral cyanosis is the normal vasoconstriction resulting from exposure to cold air or water.
When cardiac output is low, as in severe congestive heart failure or shock, cutaneous vasoconstriction occurs as a compensatory mechanism so that blood is diverted from the skin to more vital areas such as the central nervous system and heart, and intense cyanosis associated with cool extremities may result.
Even though the arterial blood is normally saturated, the reduced volume flow through the skin and the reduced PO2 at the venous end of the capillary result in cyanosis.
Arterial obstruction to an extremity, as with an embolus, or arteriolar(小动脉的) constriction, as in cold-induced vasospasm血管痉挛(Raynaud’s phenomenon), generally results in pallor(苍白) and coldness, but there may be associated with cyanosis. Venous obstruction, as in thrombophlebitis(血栓性静脉炎), dilates the subpapillary venous plexuses(丛) and thereby intensifies cyanosis.