Download
1 / 37

E N D
Renal 1 October 2, 2013 Lecturer: Dr. Sved
Claude Bernard: "It is the fixity of the internal environment that is the condition of free and independent life.... All vital mechanisms, however varied they may be, have only one object, that of preserving constant conditions of life in the internal environment".
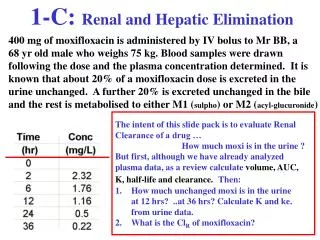
Water Loss by the Kidneys. The remaining water loss from the body occurs in the urine excreted by the kidneys. There are multiple mechanisms that control the rate of urine excretion. In fact, the most important means by which the body maintains a balance between water intake and output, as well as a balance between intake and output of most electrolytes in the body, is by controlling the rates at which the kidneys excrete these substances. For example, urine volume can be as low as 0.5 L/day in a dehydrated person or as high as 20 L/day in a person who has been drinking tremendous amounts of water. The insensible water loss through the skin occurs independently of sweating and is present even in people who are born without sweat glands; the average water loss by diffusion through the skin is about 300 to 400 ml/day. This loss is minimized by the cholesterol-filled cornified layer of the skin, which provides a barrier against excessive loss by diffusion. When the cornified layer becomes denuded, as occurs with extensive burns, the rate of evaporation can increase as much as 10-fold, to 3 to 5 L/day. For this reason, burn victims must be given large amounts of fluid, usually intravenously, to balance fluid loss. Insensible water loss through the respiratory tract averages about 300 to 400 ml/day. As air enters the respiratory tract, it becomes saturated with moisture, to a vapor pressure of about 47 mm Hg, before it is expelled. Because the vapor pressure of the inspired air is usually less than 47 mm Hg, water is continuously lost through the lungs with respiration. In cold weather, the atmospheric vapor pressure decreases to nearly 0, causing an even greater loss of water from the lungs as the temperature decreases. This explains the dry feeling in the respiratory passages in cold weather. This variability of intake is also true for most of the electrolytes of the body, such as sodium, chloride, and potassium. In some people, sodium intake may be as low as 20 mEq/day, whereas in others, sodium intake may be as high as 300 to 500 mEq/day. The kidneys are faced with the task of adjusting the excretion rate of water and electrolytes to match precisely the intake of these substances, as well as compensating for excessive losses of fluids and electrolytes that occur in certain disease states. In Chapters 26 through 30, we discuss the mechanisms that allow the kidneys to perform these remarkable tasks. Insensible Water Loss. Some of the water losses cannot be precisely regulated. For example, there is a continuous loss of water by evaporation from the respiratory tract and diffusion through the skin, which together account for about 700 ml/day of water loss under normal conditions. This is termed insensible water loss because we are not consciously aware of it, even though it occurs continually in all living humans. Fluid Loss in Sweat. The amount of water lost by sweating is highly variable, depending on physical activity and environmental temperature. The volume of sweat normally is about 100 ml/day, but in very hot weather or during heavy exercise, water loss in sweat occasionally increases to 1 to 2 L/hour. This would rapidly deplete the body fluids if intake were not also increased by activating the thirst mechanism discussed in Chapter 29. Normal Prolonged, Heavy Exercise Water Loss in Feces. Only a small amount of water (100 ml/day) normally is lost in the feces. This can increase to several liters a day in people with severe diarrhea. For this reason, severe diarrhea can be life threatening if not corrected within a few days. Figure 25-1 Summary of body fluid regulation, including the major body fluid compartments and the membranes that separate these compartments. The values shown are for an average 70-kilogram person. Daily Loss of Body Water Table 25-1. Daily Intake and Output of Water (ml/day) Link to this page: http://www.studentconsult.com/content/default.cfm?ISBN=0721602401&ID=HC025003 pages 291 - 292 page 291 page 292 Total output Intake Total intake Insensible-skin Fluids ingested Output Sweat Feces Urine From metabolism Insensible-lungs 1400 2300 5000 6600 2300 2100 500 200 200 350 350 100 100 100 650 350 ? ? Balance: matching input and output Guyton and Hall table 25-1
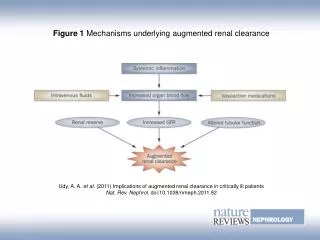
Functions of the Kidneys • Excretion of metabolic wastes • Excretion of foreign substances (e.g., toxins, drugs) • Regulation of body fluid osmolality • Regulation of electrolyte concentrations (e.g., Na+, K+, Ca++) • Maintenance of water balance and electrolyte balance • Contributes to maintenance of body pH • Regulation of erythrocyte number (erythropoietin) • Regulation of blood pressure • Glucose production
~1,000,000 nephrons per kidney; 75% cortical and 25% juxtamedullary
Urinary excretion rate = filtration rate – reabsorption rate + secretion rate From Silverthorn
So, for each substance: • To what extent is it filtered in the glomeruli? • Is it reabsorbed? (if so, where? how>?) • Is it secreted? (if so, where? How?) • What factors homeostatically regulate these processes
Brief overview of transport of molecules across membranes • There are essentially 4 ways the molecules get across membranes: • Simple diffusion (limited to lipid soluble substances) • Simple diffusion through holes (i.e., pores) (limited to select ions) • Carrier-mediated transport • Endocytosis/exocytosis
Three factors influence mediated transport: • Relative affinity of the ligand for the transporter • How many transporters • How fast the transporter works Note: transport maximum; competition
Mediated transport can be divided into two categories based on whether or not energy is required • Facilitated diffusion • Active transport • Primary • Secondary
Facilitated diffusion Simple diffusion Active transport [Ci = Co] [Ci] time time time Flux [Co]
And don’t forget about the movement of water!! • Osmosis The net diffusion of water down its own concentration gradient • Movement through water channels (aquaporins) • Understand osmotic pressure
Filtration = net filtration pressure X Kf From Silverthorn
3 filtration layers: • Capillary endothelial cells (highly fenestrated) • Basal lamina (non-cellular protein matrix) • podocytes From Widmaier
FIGURE 1. Renal glomerular filtration systemEach human kidney contains ~1,000,000 glomeruli. An afferent arteriole branches into capillaries (glomerular tuft), the walls of which constitute the glomerular filter. The plasma filtrate, the primary urine, is led to the proximal tubules while unfiltrated blood is returned to the blood circulation. The filtration barrier contains fenestrated endothelial cells, the glomerular basement membrane (GBM), and podocytes with their interdigitating foot processes. The slit diaphragm is uniformly wide, porous filter structure containing specific components. Tryggvason K, Wartiovaara J. How does the kidney filter plasma? Physiology (Bethesda). 2005 Apr;20:96-101.
a | Glomerular filtration occurs through the capillary wall into the urinary space, which empties into the proximal tubules. b | The capillary wall contains an innermost fenestrated endothelium, the GBM, and a layer of podocytes with interdigitating foot processes. c | Podocyte foot processes, interconnected by slit diaphragms, form the final barrier for filtration. Proteins that anchor the foot processes to the GBM ( 3 1 integrin, ACTN4, ILK and the tetraspanin CD151) as well as those that are associated with the slit diaphragm (nephrin, NEPH1, podocin, Fat1, ACTN4, the adaptor protein NCK, CD2AP, and TRPC6) are crucial for normal function of the filtration barrier. Abbreviations: ACTN4, -actinin-4; CD2AP, CD2-associated protein; GBM, glomerular basement membrane; ILK, integrin-linked kinase; P, podocin; TRPC6, transient receptor potential cation channel 6. [Note: I don’t expect you to remember these proteins, only that the structure of the slit diaphragm is highly complex.] Patrakka J, Tryggvason K. New insights into the role of podocytes in proteinuria. Nat Rev Nephrol. 2009 Aug;5(8):463-8.
Although we don’t normally think of Kf being a regulated variable, the mesangial cells might act to regulate the size of the podocyte filtration slits
Let’s consider what contributes to net filtration pressure: • Pressure inside Bowmans capsule (~ 15 mm Hg) doesn’t change much, unless there is an obstruction in the tubule system • Capillary pressure can change: regulation by afferent and efferent arterioles
Impact of afferent and efferent arteriole changes on GFR Silverthorn Figure 19-8 - Overview
Glomerular filtration rate • 125 ml/min; 180 L/day • In terms of Na, ~3.5g/L so the filtered load is 630G/day
GFR is stable across a range of blood pressures - Renal Autoregulation!!
Two mechanisms contribute to autoregulation: • Myogenic control (increased pressure causes arterioles to contract) • Tubuloglomerular feedback (Na delivery to distal tubule is ‘sensed’ in the macula densa, which influences the afferent and efferent arterioles)
Tubuloglomerular feedback Paracrine signaling Endocrine signaling
Consider a substance in blood that is filtered but neither reabsorbed or secreted; it is subsequently excreted: GFR X Ps = Us X V (where Ps is the plasma concentration of the substance, Us is the urinary concentration of the substance, and V is the urine volume) so we could determine GFR by: GFR = V X Us / Ps (provided that the substance is filtered but neither reabsorbed or secreted)
schematic illustrating the clearance of inulin, and how it relates to GFR Figure 19-16