Download
1 / 37
370 likes | 510 Vues
Can Markets for Health Insurance Work?. Jonathan Levin Gaston Eyskens Lectures November 2013. Roadmap. Lectures Technology and Asymmetric Information High Risk Consumer Credit Markets Measuring Inefficiencies from Adverse Selection Can Markets for Health Insurance Work?. Introduction.

E N D
Can Markets for Health Insurance Work? Jonathan Levin Gaston Eyskens Lectures November 2013
Roadmap Lectures • Technology and Asymmetric Information • High Risk Consumer Credit Markets • Measuring Inefficiencies from Adverse Selection • Can Markets for Health Insurance Work?
Introduction • Arrow (1960): healthcare as an industry where traditional notions of competition and efficiency are problematic. • Why? Uncertainty and asymmetric information. • Needs are concentrated => must have insurance • Potential for adverse selection in insurance • Moral hazard for insured individuals • Physicians asymmetrically informed about care • How well can markets for health insurance work? Should there be a major role for private market competition in a national healthcare system?
Private Market Solutions • Of developed countries, US has perhaps the most “privatized” healthcare / health insurance system. Source: OECD • It also has the most expensive system.
What Role for Markets? • Major debate in the United States, where healthcare is 18 percent of GDP, and 21 percent of federal budget. • Medicare (over 65) • Private market insurance now offered as a substitute for government insurance. Republicans propose to shift entirely to “premium support”. • Obama Health Insurance Reform (under 65) • Attempts to provide universal coverage by mandating the purchase of (subsidized) insurance, and establishing state insurance exchanges. • Some parallel debates in European countries.
Outline of Lecture • Describe research with Jay Bhattacharya, Vilsa Curto, LiranEinavon Medicare’s experiment with managed competition. • Motivation: current structure of US Medicare program is opportunity to compare two public / private systems operating head-to-head, fixing the population and set of healthcare providers. • Outline of lecture • Medicare and managed competition • Risk selection • Imperfect competition • Market design • Caveat: work in progress….
Background on US Medicare Program • Medicare program is government provided health insurance for all those over 65, plus disabled, ESRD, etc. • Individuals pay modest (≈$100) monthly premium. • Insurance covers hospital and outpatient services. • Privatized drug coverage introduced in 2006. • Traditional “fee for service” insurance (FFS) • Beneficiaries can use any doctor or hospital that accepts Medicare. Most do. Medicare reimburses for services. • Price for each service is set administratively, plus there are a complex set of hospital / facility subsidies.
Concerns about Medicare • Widely viewed as very inefficient • Why? Low copayments + physician incentives to “do more” => overuse of services. No constraints on spending / utilization. • Many documented distortions due to administrative pricing, e.g. bias towards procedures, specialists. • Striking geographic variation in costs • Medicare spends $13,824 to provide healthcare to someone in McAllen, TX, versus $7,766 in Rochester. • Common interpretation: indicates wide scope to provide different services, and lack of cost-efficient “standards” of care.
Medicare Advantage Program • US introduced private plans in 1985: beneficiaries could opt out of traditional insurance, and enroll in a private insurance plan. • Approved plans receive annual payment for each enrollee, initially 95% of local FFS costs, and updated periodically. • Hope was that private plans would allow consumer flexibility, save taxpayer dollars, and preserve quality. • But there were problems … • Low take-up – less than 15% of beneficiaries as of 2003 • Evidence of significant risk selection (cream-skimming) • Projected cost savings were not realized
Managed Competition • In 2003, new legislation introduced competitive bidding. • Attempt to avoid setting administrative capitation rates. • Risk adjustment added to address selection. • Based on proposals that date back to the 1970s. Some similarities to proposed state exchanges. • Risk adjustment developed between 2003-2006. • Every Medicare beneficiary scored based on disease history. • Regression model used to map diseases into predicted cost.
Questions • Selection • Do private plans manage to select relatively healthy enrollees? Is risk-adjustment successful in addressing this? • Competition • Is bidding competitive? Do bids reflect underlying costs, or does the program create substantial insurer rents? • Further questions about quality, innovation, cost growth, efficacy of consumer choices, etc..
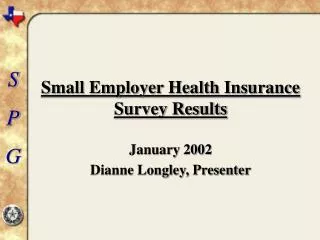
Selection: enrollment by risk score High risk beneficiaries are less likely to enroll in private plans.
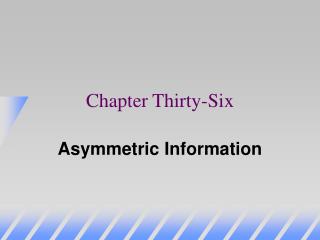
Selection: conditional on risk score Mortality notably lower among new MA enrollees.
Disease Classification Incentives Private plans are more aggressive in coding diseases.
Adjusting for Selection & Up-coding • For each private plan enrollee, we observe plan’s bid and payment, and can impute an FFS cost based on county and risk score. • Up-coding and selection adjustments (still somewhat ad hoc): • Disease classification: MA risk scores higher by 2-5% (?) • Selection: based on mortality + lagged MA costs => 1-4% (?)
Competition and Market Concentration • Medicare Advantage market is highly concentrated • We need to take imperfect competition seriously.
Medicare Advantage Rules • Country divided into local markets (3,034 counties). • Medicare sets benchmark rateB for each county. • Plans bid to provide “standard” insurance for a “standard” individual. • Individuals choose a plan in their market, or standard Medicare. Benchmark Plan Cost $ b c B b CMS pays plan b Enrollee pays 0 CMS pays plan B Enrollee pays b-B And CMS pays plan a “rebate” ¾*(B-b) that it passes to consumer in as higher benefits. • Consumer “price”:
Benchmarks and Bidding Incentives • Plan demand depends on . • Plan profits • Benchmark plays the role of a subsidy. • Under “perfect” competition with , .
Empirical Model of Plan Bids • Empirical model of plan j bid in year t. • A single plan bid may apply to several counties=>define • Plan benchmark = average of county benchmarks in a plan’s service area (using plan enrollment to weight). • Plan costs = average FFS costs for an r=1 individual in plan’s service area (again, plan enrollment to weight).
Implications of Bid Estimates • Bids are highly responsive to benchmarks, but not closely related to FFS costs (conditional on B). • Suggestive of market power… • Ideally, would like to estimate private plan margins . • Local TM costs don’t appear be a good proxy for . • Directly measure utilization? Might be possible … not today. • Estimate demand and infer from profit-maximization.
Estimating Plan Demand • Assume i’s utility for plan j in county-year (market) m is • Imposing a logit error gives us the demand model • where Xs are plan and market characteristicsand we use in place of premium, with effect varying on
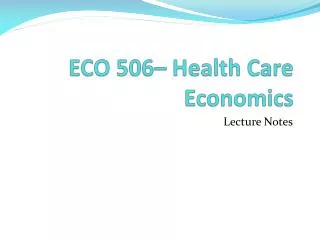
Demand Elasticity Estimates Includes characteristics: plan star rating, indicators for part D & supplementary benefits.
Inferring Margins • Profit-maximization • Average bid is , so margins are • Cutting margins in half would save $10 bn a year. • Could these savings be realized? How? • Better rebate design (current DWL) • Lower benchmarks (competition with TM) • Better choice guidance for consumer (star ratings!) • Entry and greater competition
Market Design: Rebates • Insurer that bids receives rebate of . • Typically used to provide more generous insurance. • Why not pass the rebate directly to enrollees in cash? • Logistically challenging under current rules. • Estimates say elasticity increases => margins of $71, not $125. • What about increasing/decreasing the rebate? • If rebate then margins = $62, but taxpayers always pay … this is the premium support model Republicans want. • By lowering rebate, e.g. to 50%, reduces taxpayer cost with fixed bids, but reduces incentives for insurers to lower their bids.
Market Design: Benchmarks • County benchmarks are main design parameter • If bids track benchmark, then lower B means lower margins. • However, entry is also responsive to market benchmarks. • Back of envelope calculation. A $100 decrease in benchmark: • directly decreases bids by $50 • but maybe plans would exit?
Choosing Benchmarks • County benchmarks are main design parameter • If bids track benchmark, then lower B means lower margins. • However, entry is also responsive to market benchmarks. • Back of envelope calculation. A $100 decrease in benchmark: • directly decreases bids by $50 • induces exit of 3.5 plans, which increases bids, but by < $5 • Based on our estimates (including margins of > $100 per month per enrollee) desirable to reduce benchmarks. • We are about to try this under Obamacare.
Prospects for Competition • Are private plans competing with each other, or the government? • MA/TM enrollment transitions, 2006-2010 • In markets with low private plan penetration, traditional government insurance is the primary competition. • (Note: choices also are pretty persistent … switching costs?)
Public “Option” as Constraint • Option to use TM appears to be an important constraint on plan bids, especially in areas with low penetration / few plans. • Interestingly, the Obamacare reform does not include a public option for insurance, although some lobbied for it. • One hypothesis is that private plan competition may not work all that well in low entry (likely rural) markets.
Conclusions • US is engaging in a huge national experiment with managed competition provision of health insurance. • Ongoing Medicare private plan program has grown rapidly, but at what appears to be fairly significant cost to taxpayers. • There do appear to be potential cost savings; the question is whether it is possible to realize them. • We have started to look a few possible mechanisms, but project is still at a fairly early stage…