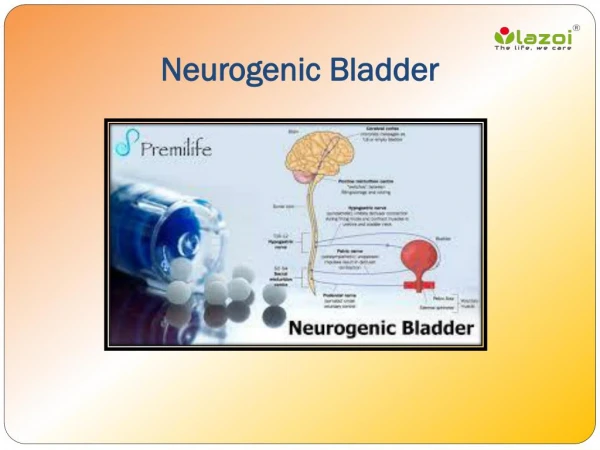
Neurogenic Bladder
Neurogenic Bladder. Ayman Mahdy,MD, PhD Associate Professor of Surgery Division of Urology Director Voiding Dysfunction and Female Urology UC. Anatomy and physiology . Bladder wall : smooth muscle/3 layers Urethral sphincter: Internal/involuntary /smooth part: BN

Neurogenic Bladder
E N D
Presentation Transcript
Neurogenic Bladder Ayman Mahdy,MD, PhD Associate Professor of Surgery Division of Urology Director Voiding Dysfunction and Female Urology UC
Anatomy and physiology • Bladder wall : smooth muscle/3 layers • Urethral sphincter: • Internal/involuntary /smooth part: BN • External/voluntary/striated part: mid urethra • Spinal cord ends at L1/L2 vertebral level • Lower urinary tract nerve supply: • Parasympathetic : S2-S4 spinal segments • Sympathetic: T10-L2 spinal segments • Somatic: S2-4 (Pudendal N) • Two types of the afferent nerves within the pelvic nerves: A and C (Morrison JW 1986).
Urine Storage Sensory perception Inhibition Medial pontine micturation center Lateral pontine micturation center Lateral Spinothalamic tract Stimulation of sympathetic neurons Sacral cord Inhibit sacral parathympathetic Stimulate sacral somatic Contraction SS and bladder outlet Dorsal ganglion Contraction of sphincter Relaxation of detrusor Receptors in muscle wall and mucosa
Micturation reflex Sensory perception facilitation Medial pontine micturation center Medial pontine micturation center Lateral Spinothalamic tract Stimulate sacral parathympathetic Inhibit sacral somatic Sacral cord Dorsal ganglion Receptors in muscle wall and mucosa Contraction of detrusor Relaxation of sphincter
What is NGB? Any bladder abnormality of micturation caused by neuromuscular disease, injury or dysfunction
Most common patterns of NGB with different neurological disease
Most common patterns of NGB with different neurological disease
Obstructive LUTS • Hesitancy • Slow stream • Intermittency • Straining to void • Spraying (splitting) of urinary stream • Feeling of incomplete (bladder) emptying • Need to immediately re-void • Post-micturition leakage • Position-dependent micturition • Dysuria • Urinary retention
Storage LUTS • Urinary frequency • Urinary urgency • Nocturia • OAB , urgency syndrome
Urinary incontinence • Stress UI • Urgency UI • Postural UI • Nocturnal enuresis • Mixed UI • Continuous UI • Insensible UI • Coital UI
Dynamics of voiding dysfunction • Bladder • Bladder outlet • Both Male Female
Dynamics of obstructive LUTS • Bladder: • Weak or absent detrusor contraction e.g. diabetic cystopathy • Bladder outlet: • Bladder outlet obstruction e.g. DESD • Combination
Dynamics of storage symptoms/UI • Bladder: • Detrusor overactivity (overactive bladder) • Bladder outlet: • Intrinsic sphincter deficiency • Combination Normal sphincter Incompetent sphincter
History • Urinary tract symptoms • Neurological symptoms and diagnosis (if known) • Clinical course of the neurological disease • Bowel symptoms • Sexual function • Comorbidities • Use of prescription and other medication and therapies.
History (Cont.) • Acute (reversible) UI: • Acute onset and subsides with underlying condition • Causes outside the urinary tract • DRIP: • Delirium • Restricted mobility/Retention • Infection/Inflammation/Impaction • Polyuria/Pharmaceuticals
Evaluation of voiding dysfunction in the elderly patient (Cont.) • Neurologic history: • Duration (MS and Parkinsonism) • Back surgery patients: time, level, type of lesion and affected sensation • CVA: UI before or after the onset of CVA • MS: duration, onset of exacerbations, motor deficits
P/E • Assess the impact of the underlying neurological: • Mobility • Hand function • Cognitive function
Initial management • Assure bladder emptying: • CIC • Urethral Foley • Assure hyegenic measures: • Palliative • Antimuscarinics • Timed void
Initial management (Cont.) • Refer: • Hematuria • Reurrent urinary tract infections • Hydronephrosis • kidney stones on imaging • biochemical evidence of renal deterioration.
Clean Intermittent Catheterization (CIC) • First introduced in 1972 by Lapides et al • Proffered treatment if patient has the manual dexterity • Staff support • 4-6/day • With or without anti-muscarinic use • Poor candidates: • Cognitive and physical factors • Lack of support • Deformities • Anatomical
Clean Intermittent Catheterization (CIC) • Incidence of bacteruria 1-3% catheterization • 1-4 Bacteruria/100 catheterization • Use of antibiotic prophylaxis is controversial
Indwelling catheter • Higher risk for: • Renal failure • Bladder stones • UTIs • Bladder cancer
Suprapubic tube versus urethral Foley • Easy to exchange • Avoid urethral trauma • Sexual function • Less EO in male
Autonomic Dysrelflexia • SCI above T6 • Loss of supraspinal inhibition of throaco-lumbar sympathetic outflow • Massive discharge of the sympathetic system • Clinically: • Sweating and cutaneous flushing • Pounding H/A, nasal congestion, piloerection • HTN (may be life threatening) • Bradycardia
Autonomic Dysrelflexia Textbook of NGB 2008
Autonomic Dysrelflexia: Treatment • Remove the stimulus!! • Other: • Nifedipine
Long term management • Usually 3 months after the episode • Sooner if: • Renal function deterioration • Hematuria • Hydronephrosis • Renal stones • Recurrent UTIs
Goals of Evaluation/Management • Prevent upper tract deterioration • Restore hygiene and social acceptance (UI) • Assure efficient bladder emptying • Avoid NGB bladder related complications
Complications of NGB • UTI • VURD • STONES • Renal amyloidosis (rare) • ED • Autonomic dysreflexia
Office Requirements • Handicap accessibility • Cystoscopy • VUDS • EMG • Crash Cart • Ostomy care • Multi-team members
Work up • History • Voiding diary • QOL assessment • PE • Neurological exam • Urine bacteriologic studies • RFTs • Radiologic evaluation • Upper tract • Lower tract • UDS/VUDS • Endoscopic examination
Filling No leak Stop filling Resume filling No leak
Antimuscarinics • *Benefits: • Improve compliance • Relieve frequency, urgency and UUI • Decrease intra-vesical pressure • Decrease DO • Helps protect the upper tract from deterioration *(Storher M et al 2007, Amend B et al 2008 and Kim YH et al 1997)
Antimuscarinics (Cont.) • Higher doses are usually needed in NGB population compared with non neurogenic OAB • Constipation • Dry mouth • Patients with CNS disease (impaired cognition with oxybutinin): • Darifenacin • Trospium
Treatment algorithm of OAB/UUI Initial Screening Voiding Diary Urodynamic Workup R/O Obstruction Interstim Interstim Behavioral Techniques Biofeedback Medications - Botox Neurostimulators Other Surgical Intervention Botox Urgent PC
Botulinum toxin A (Botox) • FDA approved 2011 for 200 unites • In patient with neurogenic detrusor overactivity • Indications: • Antimuscarinic drugs ineffective or poorly tolerated. • Medication cost • Compliance • Two RCT proved efficacy • Mean duration of effect 36-42 weeks
Surgical treatment • Sphicterotomy • Bladder augmentation • Urinary diversion: • Continent • Incontinent