CASCADE: AIDS or death
170 likes | 332 Vues
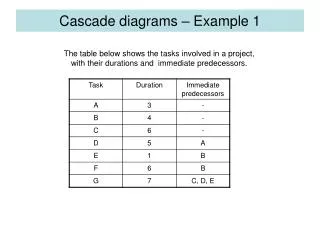
When to start antiretroviral therapy Julian Elliott Department of Infectious Diseases, Alfred Hospital and Monash University Centre for Population Health, Burnet Institute Melbourne ASHM Early Treatment Webinar, Melbourne, March 2014. CASCADE: AIDS or death. D:A:D Study:

CASCADE: AIDS or death
E N D
Presentation Transcript
When to start antiretroviral therapyJulian Elliott Department of Infectious Diseases, Alfred Hospital and Monash University Centre for Population Health, Burnet Institute MelbourneASHM Early Treatment Webinar, Melbourne, March 2014
CASCADE: AIDS or death D:A:D Study: Estimated incidence of CKD (≤60 mL/min) = 1.33 cases / 1000 person years = 0.4% over 3 years 30.0 15.0 4.8 + 0.3 2.9 Ryom et al. J Infect Dis 2013;207:1359-69 CASCADE Collaboration. Arch Intern Med 2011;171:1560-1569
Principles • All people with HIV should consider commencing ART. • Clinicians should regularly discuss the current state of knowledge regarding when to start ART with all individuals with HIV who are not yet on treatment. • All decisions to start ART should be made by the individual with HIV, in consultation with their health care providers and on the basis that they are fully informed and supported in their decision making. • The decision to start ART should take into account both personal health benefits and risks, and reduction in transmission risk.
Individuals with CD4 count < 350 • Strong evidence from randomised trials that ART reduces morbidity and mortality ART is strongly recommended
Individuals with CD4 count 350 - 500 • Moderate evidence from observational studies that ART is associated with reduced morbidity and mortality ART is recommended following discussion of the limitations of the current knowledge of benefits and risks
Individuals with CD4 count > 500 • Limited evidence regarding the balance between the benefits and risks of ART The benefits of ART potentially outweigh the risks and should be particularly considered in the following situations • Prevention of onward transmission of HIV • Individuals > 50 years • Rapid CD4 cell decline • Hepatitis B co-infection requiring treatment for hepatitis B • Early HIV infection • HIV associated neurocognitive disorders • Malignancies requiring immunosuppressive chemotherapy or radiotherapy • Tuberculosis
Key practice points: personal health • CD4 < 350: strong evidence ART reduces mortality and morbidity. • CD4 350 – 500: moderate evidence ART reduces morbidity (and mortality). • Studies were not designed to capture all important benefits and harms • Studies may have been confounded • CD4 > 500: limited evidence of net benefit • Pathogenesis studies have documented the harm associated with HIV viraemia.
Key practice points: transmission • Heterosexuals: strong evidence ART greatly reduces HIV transmission • Particularly important for serodiscordantheterosexual couples wishing to conceive • Homosexual men: moderate evidence ART substantially reduces HIV transmission • Combination prevention approach is recommended • High and consistent adherence to ART to achieve (after several months of treatment) and maintain viral suppression • Correct and consistent use of condoms and safe infecting practices • Regular tests for STIs
Key practice points: other • Once started ART should be continued indefinitely. • Currently discordance between recommendations by key guideline groups • US (DHHS and IAS-USA): ART for all (expert opinion CD4 > 500) • UK (BHIVA): ART if CD4 < 350 • EU (EACS); WHO and AUS (ASHM): ART if CD4 < 500 • All support ART for prevention if requested by the patient. • If patients continue to be unsure encourage to seek a second opinion from an experienced HIV clinician or contact local PWHIV organisation.
Cases Prepared by David Baker
Ron – 2011 • 34 year old gay male • HIV +ve 2011 • CD4 = 570, VL = 102 000 • One partner who is HIV +ve • Not wanting treatment • Otherwise well
Ron – 2014 • No regular follow-up • Herpes zoster • CD4 = 470 • Starting ARVs
Jack • 62 year old heterosexual male • Long term HIV –ve partner • Otherwise well • CD4 = 718 • VL = 7800
Tim • 44 year old gay male • HIV +ve 2 years • Single, multiple partners • CD4 = 620 • VL = 89 000 • Weekend alcohol and crystal binges • Wants to sort out drug problem before starting treatment