Download
1 / 75
750 likes | 1.17k Vues
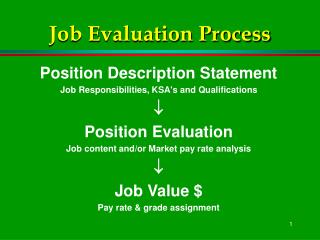
Prévention de la maladie thrombo-embolique : Position du problème en 2005 et RPC SFAR-ANAES. Charles Marc SAMAMA Département d’Anesthésie-Réanimation Hôpital Avicenne, Bobigny. levels of venographic risk when no prophylaxis is used Salzman EW, Hirsh J, THRIFT conference, 1992.

E N D
Prévention de la maladie thrombo-embolique : Position du problème en 2005 et RPC SFAR-ANAES Charles Marc SAMAMA Département d’Anesthésie-Réanimation Hôpital Avicenne, Bobigny
levels of venographic risk when no prophylaxis is usedSalzman EW, Hirsh J, THRIFT conference, 1992 DVT proximal DVT fatal PE low risk < 10% < 1% 0.01 - 0.1% moderate 10 - 40% 1 - 10% 0.1 - 1% high risk40 - 80% 10 - 30% 1 - 10%
METHODES MECANIQUES • Surélévation des membres inférieurs • Mobilisation orteils pied pied cheville jambe cuisse diaphragme • Contention élastique graduée (pied 18 mm- mollet 14 mm - genou 8 mm)
Combining compression stockings with heparin may provide better protection against VTE % thromboembolic complications Wille-Jorgensen 1985
Foot pump vs LMWH after THR prospective, randomized study - venography transfusions : NS acceptability of the pump : uncomfortable 11%; sleep disturbance 17%; 101 hrs (23-133) during 7 days; median 15 hrs each day; DVT 13%* (>15hrs) vs 21% (<15hrs) Warwick et al. J Bone Joint Surg 1998; 80A: 1158-66
DANAPAROÏDE (Orgaran®, Riom)
LMWH is effective in reducing DVT % DVT after total hip replacement Chest 1998
enquête officielle de pharmacovigilance • 1-1-97 au 30-4-99 - Comité Technique de Pharmacovigilance • Pr Montastruc (Toulouse) - interrogation de la base nationale 175 observations - 51 décès (39) - délai moyen: 12 à 14j insuffisance rénale: 15 à 40% - age >75 ans : 51 à 75% mésusage : 51 à 75%
HBPM et fractures du col 49 patients - 81±13 ans - daltéparine 5000 UI clairance initiale créatinine (Cockroft) : 35 ± 22 ml/min 10 hématomes de paroi Michaut-Paterno, SFAR 2000
pre-op , post-op LMWH, warfarin THR - randomized double blind - venography d5-6 (n=414) Dalteparin 2500 : 50 min before surgery or 7 hrs after pre-op gpe: increased major bleeding (day 0 -1, operative site 8.9% vs 4.5% warfarin gpe) - clinical DVTs ?? Hull, NAFT trial, Arch Int Med 2000
Preoperative or Postoperative Start of Prophylaxis for VenousThromboembolism with Low Molecular Weight Heparin in Elective Hip Surgery Strebel et al. Arch Int Med 2002; 162: 1451-1456 20 % 19,2 14,4 12,4 10 % 6,3 1,4 2,5 pre-op H < -12 periop (H-12+12) post-op H > 12 n = 1926 n = 925 n = 694 enoxaparin 40 mg major bleeding global venographic DVT
Seventh ACCP Consensus Conference on Antithrombotic Therapy, Chest 2004
Extended-duration prophylaxis against venous thromboembolism after total hip or knee replacement : a meta-analysis of the randomised trials Eikelboom et al, Lancet 2001; 358: 9-15 Venographic DVT 9.6% vs 19.6%% OR 0.48
Prolonged vs. In-Hospital Thromboprophylaxis with Enoxaparin after Surgery for Abdominal Malignancy (ENOXACAN II) • total treatment duration : 283 days - n = 331 patients • primary efficacy endpoint : incidence of postoperative DVT or PE enoxaparin 4.9%* vs.placebo 12.0 • combined incidence of prox. DVT and PE : 0.61% (E) to 2.4% (P) • incidence of bleeding during the double-blind period: NS enoxaparin 40 mg (21 days) enoxaparin 40 mg (8 d) venography day 28 placebo (21 days)
long term prophylaxis : the SACRE study oral anticoagulant (Sintrom®) - 2<INR<3 5 days THR OAC + LMWHor LMWH LMWH (Clivarine®) - 4200 IUAxA 6 weeks - clinical endpoint (DVT and pulmonary embolism and bleeding)
SACRE : évènements - population ITT Samama et al., Arch Int Med 2002
levels of venographic risk when no prophylaxis is usedSalzman EW, Hirsh J, THRIFT conference, 1992 DVT proximal DVT fatal PE low risk < 10% < 1% 0.01 - 0.1% moderate 10 - 40% 1 - 10% 0.1 - 1% high risk40 - 80% 10 - 30% 1 - 10%
Incidence and natural history of deep-vein thrombosis after total knee arthroplastyKim YH, Kim JS, JBJS 2002; 84B: 566-570 • Prospective study- 227 primaryTKR (111 unilateral, 116 bilateral) - no prophylaxis and no therapeutic treatment • Venograms D6-7 and repeated six months after operation in all patients who had thrombi • Positive venograms : bilateral replacement : 97/232 (41.8%, proximal 21.6%); unilateral 46/111 (41.4%, proximal 34.8%) • 143 venograms at six months : all thrombi had completely resolved. No PE (negative pre-and postoperative perfusion lung scans and absence of symptoms)
Incidence of symptomatic venous thromboembolism after different elective or urgent surgical proceduresWhite RH et al. Thromb Haemost 2003; 90: 446-455 Administrative data-base, 1,653,275 cases - 76 selected surgical procedures between Jan 1, 1992 and Sept 30, 1996 VTE within a 3 month period diagnosed in 13,533 cases (0.8%) 5049 pulmonary embolism (37%) Predictors of VTE included: - advancing age (OR=1.1 per 5 year increment in age) - presence of a malignancy (OR = 1.7) - prior VTE (OR = 6.2)
Enquête Française Observationnelle sur l’incidence à 3 mois des événements ThrombOemboliques veineux symptomatiques chez des patients opérés d’une prothèse totale de hanche ou de genou (FOTO) 1 770 observations dans 130 centres (2 à 57/centre) PTH : 62 % PTG : 38 % • Evénements thrombo-emboliques symptomatiques SANS dépistage à 3 mois (62% des patients) : 1080 patients et 2O évènements1,8 % (1.3% PTH, 2.8% PTG) dont seulement 2 EP non mortelles • Hémorragies majeures1,4 % • Décès 0,6%
Evènements cliniques dans les Suites d’une intervention Chirurgicale Orthopédique à RisqueThrombotique Elevé PE DVT VTE 0.25% 0.21% 1,36% 0.14% 1,09% 0.11% 0.11% 0,99% 0,83% 0,79% 0,06% 0,54% 1,34% 0,95% 1,10% 1,23% 0,59% 0,92% 15 days 30 days 45 days 60 days 75 days 90 days VTE distribution (n=85) 45,9% (n=39) 21.2% (n=18) 2,4% (n=2) 12,9% (n=11) 9,4% (n=8) 8,2% (n=7) VTE evolution as per time 6860 evaluable patients = 70% of all patients having surgery for hip fracture over two months in France (525 centers - oct-nov 2002) Symptomatic VTE (3 months): 1.34% [1.06-1.62%] Pulmonary Embolism (3 months): 0.2%, fatal PE: 0.04% Major bleeding: 1.2%
Main causes of death at 6 months (n = 1006) 1006 deaths at 6 months (14.7%) Bleedings n=16 Cerebrovascular, (CVA, TIA, general state impairment) n=200 16% Others n=375 19,9% 38% 29% 4,1% Cardiovascular n=295 8% Pulmonary embolism n=41 Pulmonary (infection, cancer, hypoxemia, rspiratory insufficiency), n=79
quel est le bon critère ? • Taux total de thromboses chez les patients traités : • critère phlébographique : 10-37 % • critère clinique : 1-3,7 % (ESCORTE 1,3% -FOTO 1,8% - SACRE 2,3%, White 2,8%, Warwick 3,4%, Colwell 3,7%) • Faut-il traiter les images, ou les patients ? • La surestimation du risque thromboembolique pourrait conduire à l’abus d’anticoagulants (hirudine, pentasaccharide, ximelagatran)
Lésion vasculaire Plaque athérome Facteur Tissulaire VII VIIa NAPC2 ASIS-TFPI // // X Xa IX IXa Anti-IXa // Anti-Xa Pentasaccharide + AT Héparines + AT DX-9065a Prothrombinase Va - Xa Phospholipides // + F VIIIa + Phospholipides + Prothrombine // Thrombine Antithrombine Héparines Hirudine Melagatran Fibrinogène Fibrine Plaquettes Activation
2002; 359: 1715-20 Day 49- venous thromboembolism 12/1129 F vs 9/1123 E : NS Major bleeding : 42F vs 29E : p=0.11
2002; 359: 1721-26 Day 49- venous thromboembolism : 29/1126 (3%) Fonda vs 13/1128 (1%) Enox - p = 0.013 Major bleeding : 18F vs 8E : p=0.11
Turpie AGG et al. Fondaparinux versus Enoxaparin For the prevention of Venous Thrombo-embolism in Major Orthopedic Surgery A Meta-analysis of 4 randomized double-blind studies Arch Int Med 2002; 162: 1833-40 Major bleeding events : Fondaparinux 96 (2.7%)* Enoxaparin 63 (1.7%) P=0.008 excès de transfusion dans le groupe fondaparinux : 1950 versus 1864 (p=0,04)
Long term prophylaxis study : PENTHIFRA plusEriksson BI et al, Arch Int Med 2003; 163: 1337-1342 • Hip fracture - n = 656 • Randomisation D7±1, double blind • Fondaparinux (Arixtra®)vs placebo for 4 weeks • Venography : D25-D32 • 1 fatal PE and 2 non fatal PE in the placebo group • Symptomatic DVTs : 1 (0.3%) vs 9 (2.7%)* • Major bleeding : 6vs 0
The ARixtra for ThromboEmbolism prevention in a Medical Indications Study (ARTEMIS) • Randomised double blind trial • Medical patients ≥ 60 yo, acute cardiac, respiratory, infectious and inflammatory disease, and expected to remain bedridden for ≥ 4days • Fondaparinux (Arixtra®) vs placebo 6-14 days - n = 849 • Primary efficacy outcome: adjudicated VTE up to day 15 (mandatory bilateral venography - n = 644) • VTE incidence: Fondaparinux: 5,6% vs placebo 10,5% (-49.5%) (p=0.029) • Symptomatic events up to day 15: Fondaparinux: 0/429 ; placebo: 5 fatal PE among 420 patients , p=0,029 • Major bleeding : NS
Fondaparinux, prévention…. • Produit synthétique, large développement • Efficacité phlébographique… • Attention à la tolérance chez les sujets « fragiles », attention à l’ALR axiale • Début 6 à 8 heures après la fin de l’intervention • Pas de problème avec les AINS • Thrombopénies induites peu probables, mais numération des plaquettes quand même ! • Prophylaxie prolongée pour la fracture du col, très efficace contre placebo. • AMM en médecine bientôt, mais pas en réanimation
Ximélagatran : antithrombine directe par voie orale (Exanta®) ximélagatran = prodrogue Passage barrière intestinale mélagatran = molécule active (peu absorbée)
Phase III : choix du schéma initial METHRO II METHRO III HBPM MELAGATRAN / XIM. J-1 J0 J1 J-1 J-1 J0 J0 J1 J1
METHRO II METHRO III EXPRESS HBPM 3 mg 3 mg 3 mg 24 mg 24 mg 24 mg J-1 J0 J1 J-1 J-1 J0 J0 J1 J1 J-1 J-1 J0 J0 J1 J1 AMM en décembre 2003 : début post-op avec mélagatran SC 3mg deux fois par j puis ximélagatran per-os pdt 11j ???
Ximélagatran/Mélagatran : en résumé • Premier anti-thrombine directe synthétique per-os • Mécanisme original • Non-infériorité phlébographique, équivalence clinique en orthopédie (PTH - PTG) • Traitement oral 11 jours (d’abord pendant 24-48h, une injection sous cutanée matin et soir…) • Bonne tolérance quand début post-op • Pas de prophylaxie prolongée pour l’instant. Nécessaire reprise des HBPM au 12è jour
SFAR Comité des référentiels Recommandations pour la Pratique Clinique (RPC) Prévention de la maladie thrombo-embolique veineuse périopératoire et obstétricale ANAES