Download
1 / 27
270 likes | 405 Vues
Presented By: Alton R. Johnson Jr. Characterization of Self-reported Asthma in Morbidly Obese Women. Outline . Asthma Pathophysiology, epidemiology, & diagnosis Obesity Definition, trends, morbidity Obesity & asthma association Supporting evidence Summer Research Project.

E N D
Presented By: Alton R. Johnson Jr. Characterization of Self-reported Asthma in Morbidly Obese Women
Outline • Asthma • Pathophysiology, epidemiology, & diagnosis • Obesity • Definition, trends, morbidity • Obesity & asthma association • Supporting evidence • Summer Research Project
Pathophysiology Asthma Inflammation Airway Hyperresponsiveness Airway Obstruction Clinical symptoms
Epidemology of asthma • One of the most common chronic respiratory diseases • affects approx. 7% of population (22 million) (CDC, 2010) • 27% are children (>6 million) (CDC, 2010) • Associated with significant morbidity • African American children have a 250% higher hospitalization rate and a 500% higher death rate (CDC, 2010)
Asthma: Prevalence • Prevalence = (# of people with the disease) / (# of people at risk for disease + # of people with the disease) • Increasing prevalence over past 20 years (NAEPP, 2010) • Significant disparity.
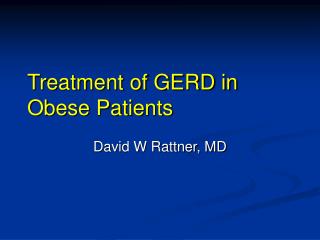
Obesity Trends* Among U.S. AdultsBRFSS,1990, 2008 (*BMI 30, or about 30 lbs. overweight for 5’4” person) 2008 1990 No Data <10% 10%–14% 15%–19% 20%–24% 25%–29% ≥30%
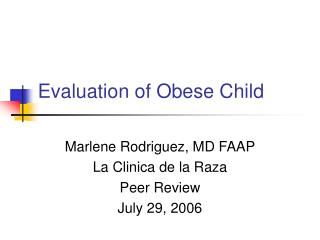
Obesity and Asthma • Cross-sectional studies • Increased prevalence of asthma in obese patients • Obesity associated with worst asthma control and increased morbidity (severe symptoms) • Longitudinal studies • Asthma risk increases by 50 % in overweight and obese people • AHR is associated with increased BMI
Obesity associated with increased risk of asthma Beuther and Sutherland 2007
Obesity and Asthma • Possible explanations: • Causal link • Obesity leads to increased risk of asthma • Inflammatory pathway • Mechanical pathway • Coincidental • Epiphenomenon • Shared risk factors (i.e. genetic, environmental) • Diagnostic bias
Effects of obesity on asthma control/severity • Controversial findings • Some studies showing worst asthma symptoms in obese patients (Schacteret.al. 2001) • Others have not (Clerisme-Beatyet.al. 2009) • Limited by use of self-report or questionnaire to diagnose asthma
Project Importance • Obesity is associated with changes in lung volumes which may mimic asthma. • It is unclear whether the asthma phenotype is different in obese patients
Objective • To examine differences in pulmonary function profile, respiratory symptoms, and quality of life in morbidly obese women based on self-reported asthma.
Recruitment • 53 participants were recruited to participate in the study. • 11 were excluded based on gender, leaving 42 women in the final analysis.
Air Hyperresponsiveness • 24 participants (6 asthmatics, 18 non-asthmatics) • 60% asthmatics had positive AHR • 40% non-asthmatics had positive AHR
Conclusions • Both Groups: • Decreased quality of life • Increased reports of respiratory symptoms • Trend for lower FEV1/FVC • Asthmatics: • Significantly more respiratory complaints • Lower quality of life • Symptoms rather than objective differences in respiratory function may guide the diagnosis of asthma in this population
Limitation • It is unclear whether these findings apply to men or patients with less severe obesity.
Acknowledgements • Emmanuelle Clerisme-Beaty, MD MHS • Mercedes Proctor, BA • Andrew Bilderback, MS • Cynthia Rand, PhD • FlonaRedway, PhD • Denise Guise Funding: • NIH/NHLBI grant R25 HL084762, Johns Hopkins University • NIH grant K12RR01767, Johns Hopkins University • NIH-NIGMS RISE Grant, R25 GM059244-09, Barry University