Download
1 / 1
10 likes | 168 Vues
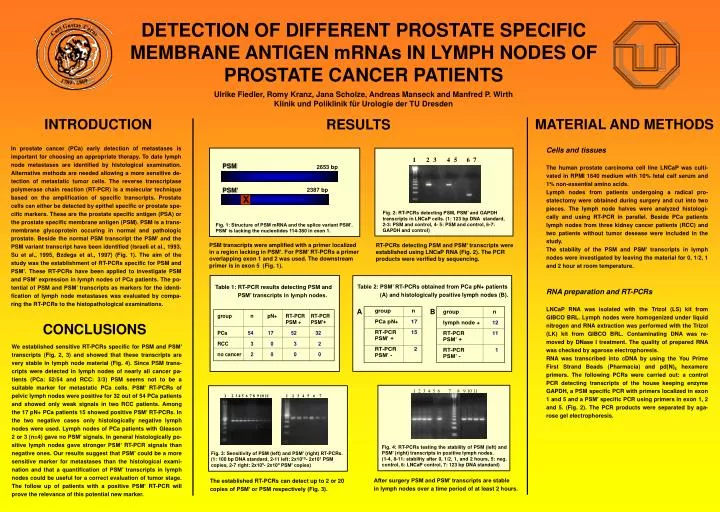
1. 2. 3. 4. 5. 6. 7. DETECTION OF DIFFERENT PROSTATE SPECIFIC MEMBRANE ANTIGEN mRNAs IN LYMPH NODES OF PROSTATE CANCER PATIENTS. Ulrike Fiedler, Romy Kranz, Jana Scholze, Andreas Manseck and Manfred P. Wirth Klinik und Poliklinik für Urologie der TU Dresden. INTRODUCTION. RESULTS.

E N D
1 2 3 4 5 6 7 DETECTION OF DIFFERENT PROSTATE SPECIFIC MEMBRANE ANTIGEN mRNAs IN LYMPH NODES OF PROSTATE CANCER PATIENTS Ulrike Fiedler, Romy Kranz, Jana Scholze, Andreas Manseck and Manfred P. Wirth Klinik und Poliklinik für Urologie der TU Dresden INTRODUCTION RESULTS MATERIAL AND METHODS In prostate cancer (PCa) early detection of metastases is important for choosing an appropriate therapy. To date lymph node metastases are identified by histological examination. Alternative methods are needed allowing a more sensitive de-tection of metastatic tumor cells. The reverse transcriptase polymerase chain reaction (RT-PCR) is a molecular technique based on the amplification of specific transcripts. Prostate cells can either be detected by epithel specific or prostate spe-cific markers. These are the prostate specific antigen (PSA) or the prostate specific membrane antigen (PSM). PSM is a trans-membrane glycoprotein occuring in normal and pathologic prostate. Beside the normal PSM transcript the PSM’ and the PSM variant transcript have been identified (Israeli et al., 1993, Su et al., 1995, Bzdega et al., 1997) (Fig. 1). The aim of the study was the establishment of RT-PCRs specific for PSM and PSM’. These RT-PCRs have been applied to investigate PSM and PSM’ expression in lymph nodes of PCa patients. The po-tential of PSM and PSM’ transcripts as markers for the identi-fication of lymph node metastases was evaluated by compa-ring the RT-PCRs to the histopathological examinations. Cells and tissues The human prostate carcinoma cell line LNCaP was culti-vated in RPMI 1640 medium with 10% fetal calf serum and 1% non-essential amino acids. Lymph nodes from patients undergoing a radical pro-statectomy were obtained during surgery and cut into two pieces. The lymph node halves were analyzed histologi-cally and using RT-PCR in parallel. Beside PCa patients lymph nodes from three kidney cancer patients (RCC) and two patients without tumor desease were included in the study. The stability of the PSM and PSM’ transcripts in lymph nodes were investigated by leaving the material for 0, 1/2, 1 and 2 hour at room temperature. RNA preparation and RT-PCRs LNCaP RNA was isolated with the Trizol (LS) kit from GIBCO BRL. Lymph nodes were homogenized under liquid nitrogen and RNA extraction was performed with the Trizol (LK) kit from GIBCO BRL. Contaminating DNA was re-moved by DNase I treatment. The quality of prepared RNA was checked by agarose electrophoresis. RNA was transcribed into cDNA by using the You Prime First Strand Beads (Pharmacia) and pd(N)6 hexamere primers. The following PCRs were carried out: a control PCR detecting transcripts of the house keeping enzyme GAPDH, a PSM specific PCR with primers localized in exon 1 and 5 and a PSM’ specific PCR using primers in exon 1, 2 and 5. (Fig. 2). The PCR products were separated by aga-rose gel electrophoresis. PSM 2653 bp PSM’ 2387 bp X Fig. 2: RT-PCRs detecting PSM, PSM’ and GAPDH transcripts in LNCaP cells. (1: 123 bp DNA standard, 2-3: PSM and control, 4- 5: PSM and control, 6-7: GAPDH and control) Fig. 1: Structure of PSM mRNA and the splice variant PSM’. PSM’ is lacking the nucleotides 114-380 in exon 1. PSM transcripts were amplified with a primer localized in a region lacking in PSM’. For PSM’ RT-PCRs a primer overlapping exon 1 and 2 was used. The downstream primer is in exon 5 (Fig. 1). RT-PCRs detecting PSM and PSM’ transcripts were established using LNCaP RNA (Fig. 2). The PCR products were verified by sequencing. Table 2: PSM’ RT-PCRs obtained from PCa pN+ patients (A) and histologically positive lymph nodes (B). Table 1: RT-PCR results detecting PSM and PSM’ transcripts in lymph nodes. B A CONCLUSIONS We established sensitive RT-PCRs specific for PSM and PSM’ transcripts (Fig. 2, 3) and showed that these transcripts are very stable in lymph node material (Fig. 4). Since PSM trans-cripts were detected in lymph nodes of nearly all cancer pa-tients (PCa: 52/54 and RCC: 3/3) PSM seems not to be a suitable marker for metastatic PCa cells. PSM’ RT-PCRs of pelvic lymph nodes were positive for 32 out of 54 PCa patients and showed only weak signals in two RCC patients. Among the 17 pN+ PCa patients 15 showed positive PSM’ RT-PCRs. In the two negative cases only histologically negative lymph nodes were used. Lymph nodes of PCa patients with Gleason 2 or 3 (n=4) gave no PSM’ signals. In general histologically po-sitive lymph nodes gave stronger PSM’ RT-PCR signals than negative ones. Our results suggest that PSM’ could be a more sensitive marker for metastases than the histological exami-nation and that a quantification of PSM’ transcripts in lymph nodes could be useful for a correct evaluation of tumor stage. The follow up of patients with a positive PSM’ RT-PCR will prove the relevance of this potential new marker. 1 2 3 4 5 6 7 8 9 10 11 1 2 3 4 5 6 7 8 9 10 11 1 2 3 4 5 6 7 Fig. 4: RT-PCRs testing the stability of PSM (left) and PSM’ (right) transcripts in positive lymph nodes. (1-4, 8-11: stability after 0, 1/2, 1, and 2 hours, 5: neg. control, 6: LNCaP control, 7: 123 bp DNA standard) Fig. 3: Sensitivity of PSM (left) and PSM’ (right) RT-PCRs. (1: 100 bp DNA standard, 2-11 left: 2x1010- 2x101 PSM copies, 2-7 right: 2x105- 2x100 PSM’ copies) After surgery PSM and PSM’ transcripts are stable in lymph nodes over a time period of at least 2 hours. The established RT-PCRs can detect up to 2 or 20 copies of PSM’ or PSM respectively (Fig. 3).