Download

1 / 40
400 likes | 604 Vues
Case 2 (HER2 positive), v5 - July 3, 2009 - to Abraxis Medical. Key Issues in the Management of Metastatic Breast Cancer. Case. First-Line Treatment of HER2-Positive ER-Negative Metastatic Breast Cancer. Case: History. 47-year-old woman with invasive ductal carcinoma 2.0 cm Node negative

E N D
Case 2 (HER2 positive), v5 - July 3, 2009 - to Abraxis Medical Key Issues in the Management of Metastatic Breast Cancer
Case First-Line Treatment of HER2-Positive ER-Negative Metastatic Breast Cancer
Case: History • 47-year-old woman with invasive ductal carcinoma • 2.0 cm • Node negative • ER negative • HER2 positive • Treated with lumpectomy, adjuvant chemotherapy with AC x 4, and radiation • Treatment completed in June 2004
Case: Clinical Presentation • In 2007, presents with nausea and RUQ pain • CT abdomen: diffuse liver metastases; marker lesion 5.5 cm • CT chest: multiple pulmonary lung nodules all <1.0 cm • Lytic bony metastases through thoracic and lumbar spine • Mildly elevated transaminases, normal bilirubin • ECOG PS = 1 RUQ = right upper quadrant ECOG = Eastern Cooperative Oncology Group PS = performance status
Case: What Are the Treatment Options? • Taxane + trastuzumab • Vinorelbine + trastuzumab • Capecitabine + trastuzumab • Taxane + carboplatin + trastuzumab (TCH) • Other
Case: Evidence-Based Treatment Options • Randomized data: with trastuzumab • Paclitaxel and doxorubicin/cyclophosphamide • Docetaxel • Taxane and platinum • Phase II data: multiple agents + trastuzumab • Vinorelbine • Capecitabine • Gemcitabine • nab-paclitaxel
Chemotherapy + Trastuzumab for MBC that Overexpresses HER2 Slamon et al. N Engl J Med 2001 Trastuzumab + anthracycline* + cyclophosphamide (n = 143) R A N D O M I Z A T I O N No previous anthracyclines Anthracycline* + cyclophosphamide (n = 138) • MBC • HER2 overexpression • No prior CT for MBC • Measurable disease • KPS >60% • n = 469 Trastuzumab + paclitaxel (n = 92) Previous anthracyclines Paclitaxel (n = 96) CT = chemotherapy KPS = Karnofsky performance status * Doxorubicin or epirubicin Slamon DJ et al. N Engl J Med 2001;344:783-92.
First-Line Chemotherapy for HER2-Positive MBCResults Slamon et al. N Engl J Med 2001 TTP = time to progression RR = response rate Slamon DJ et al. N Engl J Med 2001;344:783-92.
First-Line Chemotherapy for HER2-Positive MBCProgression-Free Survival Slamon et al. N Engl J Med 2001 Slamon DJ et al. N Engl J Med 2001;344:783-92.
First-Line Chemotherapy for HER2-Positive MBCCardiac Dysfunction Slamon et al. N Engl J Med 2001 NYHA = New York Heart Association Slamon DJ et al. N Engl J Med 2001;344:783-92.
First-Line Chemotherapy for HER2-Positive MBCM77001: Design Trastuzumab 4 mg/kg loading dose then 2 mg/kg q wk until disease progression+ docetaxel 100 mg/m2q 3 wk 6 cycles (n = 92) R A N D O M I Z A T I O N • MBC • HER2 positive • No prior CT for MBC • No prior taxanes • Baseline LVEF >50% • n = 186 Docetaxel 100 mg/m2q 3 wk 6 cycles (n = 94) LVEF = left ventricular ejection fraction Marty M et al. J Clin Oncol 2005;23:4265-74.
First-Line Chemotherapy for HER2-Positive MBCM77001: Results * Kaplan-Meier estimate Intent-to-treat population ORR = overall response rate DR = duration of response TTP = time to progression OS = overall survival Marty M et al. J Clin Oncol 2005;23:4265-74.
First-Line Chemotherapy for HER2-Positive MBCM77001: Toxicity LVEF = left ventricular ejection fraction CHF = congestive heart failure Marty M et al. J Clin Oncol 2005;23:4265-74.
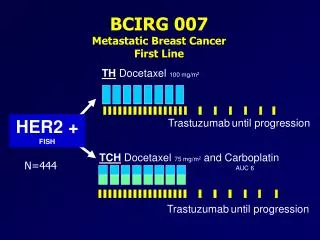
First-Line Chemotherapy for HER2-Positive MBC BCIRG 007: Taxane and Platinum 8 TH Docetaxel 100 mg/m2 q 3 wk HER2 positive by FISH n = 263 Trastuzumab* 8 TCH Docetaxel 75 mg/m2 q 3 wk Carboplatin AUC: 6 mg/mL/min Trastuzumab* • Stratification: • Prior chemotherapy • Adjuvant/neoadjuvant • Centre • Primary efficacy end point: TTP * 4 mg/kg IV, day 1, cycle 1; 2 mg/kg IV weekly starting day 8; 6 mg/kg IV q 3 wk starting 3 wk after last chemotherapy FISH = fluorescent in situ hybridization AUC = area under the curve TTP = time to progression Forbes JF et al. ASCO 2006:LBA516. Pieńkowski T et al. ESMO 2006:148PD.
First-Line Chemotherapy for HER2-Positive MBCBCIRG 007: Results CR = complete response PR = partial response SD = stable disease NC = no change PD = progressive disease NE = not evaluable RR = response rate Forbes JF et al. ASCO 2006:LBA516.
First-Line Chemotherapy for HER2-Positive MBCBCIRG 007: Time to Progression Pieńkowski T et al. ESMO 2006:148PD. Intent-to-treat population
Randomized Trials: Trastuzumab Added to Chemotherapy in First-Line MBC RR = response rate TTP = time to progression 1. Marty M et al. J Clin Oncol 2005;23:4265-74. 2. Slamon DJ et al. N Engl J Med 2001; 344:783-92. 3. Gasparini G et al. Breast Cancer Res Treat 2007;101:355-65.
Phase II Trials • Vinorelbine + trastuzumab • Capecitabine + trastuzumab • Gemcitabine + trastuzumab • nab-paclitaxel and trastuzumab
Phase II Trials: Trastuzumab Added to Chemotherapy in MBC 1. Burstein HJ et al. J Clin Oncol 2003;21:2889-95. 2. Burstein HJ et al. J Clin Oncol 2001;19:2722-30. 3. Jahanzeb M et al. Oncologist 2002;7:410-7. 4. Xu L et al. SABCS 2006:2065. RR = response rate TTP = time to progression NR = not reported 5. O’Shaughnessy JA et al. Clin Breast Cancer 2004;5:142-7. 6. Mirtsching B et al. ASCO 2008:1118.
Case: What Are the Treatment Options? • Taxane + trastuzumab • Vinorelbine + trastuzumab • Capecitabine + trastuzumab • Taxane + carboplatin + trastuzumab (TCH)
Case: Treatment • Docetaxel 100 mg/m2 • Trastuzumab • 4 mg/kg loading dose over 90 min; 2 mg/kg weekly maintenance dose over 30 min • After 2 cycles: • Liver enzymes normalize • Patient feels better
Case: Duration of Chemotherapy Treatment + Trastuzumab • Options: • Continue chemotherapy until patient has dose- limiting toxicities? • Continue chemotherapy until 2 cycles past best response? • Continue chemotherapy for 6 cycles total? • Other?
Case: Progress • Treated with 4 cycles of docetaxel then dose reduced by 20% due to neutropenia • Total of 6 cycles • Dose-limiting sensory neuropathy and peripheral edema • CT abdomen: marker liver lesion reduced from 5.5 to 2.0 cm • Continued on single-agent trastuzumab 5 months • Increasing liver enzymes • CT abdomen: progressive liver metastases
Case: Treatment Options • Stop trastuzumab and start vinorelbine • Stop trastuzumab and start capecitabine • Continue trastuzumab and start capecitabine • Initiate lapatinib + capecitabine
Trastuzumab beyond progression in human epidermal growth factor receptor 2–positive advanced breast cancer: a German Breast Group 26/ Breast International Group 03-05 study von Minckwitz G, du Bois A, Schmidt M, Maass N, Cufer T, de Jongh FE, Maartense E, Zielinski C, Kaufmann M, Bauer W, Baumann KH, Clemens MR, Duerr R, Uleer C, Andersson M, Stein RC, Nekljudova V, Loibl S von Minckwitz G et al. J Clin Oncol 2009;27:1999-2006.
GBG-26: First Randomized Phase III Study to Investigate Continuation of Trastuzumab Capecitabine 2500 mg/m2 bid days 1–14 q 21 days + continuation of trastuzumab 6 mg/kg q 3 wk (n = 78) R A N D O M I Z A T I O N Progression under taxane + trastuzumab (n = 114*) or trastuzumab monotherapy/ trastuzumab + nontaxane (n = 42) Capecitabine 2500 mg/m2 bid days 1–14 q 21 days(n = 78) • Primary end point: TTP • Study closed early (IDMC) TTP = time to progression IDMC = independent data-monitoring committee * First-line treatment for MBC: n = 111; adjuvant treatment: n = 3 von Minckwitz G et al. J Clin Oncol 2009;27:1999-2006.
GBG-26: Continuation of Trastuzumab Significantly Improves Response Rate OR: 2.50 P = 0.0115 OR = odds ratio CR = complete response PR = partial response SD = stable disease PD = progressive disease Population that received at least one cycle of allocated treatment Response to treatment not assessed: combination arm, 2.6%; capecitabine arm, 8.1% von Minckwitz G et al. J Clin Oncol 2009;27:1999-2006.
GBG-26: Progression-Free Survival Median TTP Capecitabine (X): 5.64 months (4.16–6.30) Capecitabine + trastuzumab (H): 8.16 months (7.25–11.21) Unadjusted HR*: 0.685 (0.482–0.974) P = 0.0338 (2-sided log rank) * Intent-to-treat population von Minckwitz G et al. J Clin Oncol 2009;27:1999-2006.
GBG-26: Overall Survival Median Overall Survival Capecitabine (X): 20.39 months (17.77–24.66) Capecitabine + trastuzumab (H): 25.48 months (19.02–30.69) Unadjusted HR*: 0.763 (0.477–1.220) P = 0.2570 (2-sided log rank) * Intent-to-treat population von Minckwitz G et al. J Clin Oncol 2009;27:1999-2006.
Lapatinib: Mechanism of Action Activation blocked by lapatinib Normal activation by ATP ErbB1 ErbB2 ErbB1 ErbB2 Lapatinib ATP Shc Ras Sos Grb2 Raf PI3K Akt MAPK P Akt MAPK Survival pathway Proliferation pathway Proliferation pathway Survival pathway Image: GlaxoSmithKline
Phase III Trial of Capecitabine ± Lapatinib in Advanced or MBC Geyer et al. N Engl J Med 2006 Lapatinib 1250 mg/day po Capecitabine 2000 mg/m2/day, days 1–14 q 21 days (n = 163) Median trastuzumab-discontinuation time = 5.3 wk R A N D O M I Z A T I O N • Stage IIIB or IIIC with T4 lesion, or MBC that has progressed • HER2 positive (IHC 3+ or 2+ with FISH) • Unlimited prior therapies, but no prior capecitabine • Prior therapies must include: • Trastuzumab in metastatic setting • Anthracycline and taxane in either metastatic or adjuvant setting Capecitabine 2500 mg/m2/day, days 1–14 q 21 days (n = 161) Median trastuzumab-discontinuation time = 6.0 wk IHC = immunohistochemistry FISH = fluorescent in situ hybridization TTP = time to progression PFS = progression-free survival OS = overall survival ORR = overall response rate • Primary end point: TTP • Secondary end points: PFS, OS, ORR, rate of clinical benefit, and safety Geyer CE et al. N Engl J Med 2006;355:2733-43.
Phase III Trial of Capecitabine ± Lapatinib in Advanced or MBC: TTP Cameron et al. Breast Cancer Res Treat 2008 (n = 198) (n = 201) Cumulative progression free (%) HR = hazard ratio CI = confidence interval TTP = time to progression Weeks Intention-to-treat population Cameron D et al. Breast Cancer Res Treat 2008;112:533-43.
Phase III Trial of Capecitabine ± Lapatinib in Advanced or MBC: Overall Efficacy Cameron et al. Breast Cancer Res Treat 2008 Independent assessment, intent-to-treat population * End points based on evaluation by the independent review committee under blinded conditions † Calculated with log-rank test ‡ Calculated with Fisher’s exact test HR = hazard ratio PFS = progression-free survival ORR = overall response rate CI = confidence interval CR = complete response PR = partial response SD = stable disease Cameron D et al. Breast Cancer Res Treat 2008;112:533-43.
Toxicity Cameron et al. Breast Cancer Res Treat 2008 Patients (%) L = lapatinib C = capecitabine PPE = palmar plantar erythrodysesthesia Cameron D et al. Breast Cancer Res Treat 2008;112:533-43.
Summary • Suppressing HER2 upon progression appears to continue to benefit • Either continue trastuzumab with a change in chemotherapy or switch to lapatinib
Case: Progress • Continued trastuzumab • 4 mg/kg loading dose over 90 min; 2 mg/kg weekly maintenance dose over 30 min • Started capecitabine 2000 mg/m2 bid • Tolerated therapy well • PR after 2 cycles PR = partial response
Challenges for Physicians in Canada • Treatment with trastuzumab beyond progression is not funded in many provinces • Lapatinib is an oral drug; coverage is not yet certain* • Capecitabine is an oral drug and is not covered in some provinces for patients <65 years without a drug plan * As of June 2009
HER2-Positive MBC Treatment Summary • For women with HER2-positive MBC, trastuzumab + chemotherapy should be the treatment of choice • Choice of chemotherapy should be individualized based on clinical presentation • Treatment options for patients who progress on trastuzumab: • Continuation of trastuzumab + other chemotherapeutic agents (phase II data) • Continuation of trastuzumab + capecitabine (phase III data) • Lapatinib + capecitabine (phase III data) • Chemotherapy alone
Treatment Summary • No gold-standard treatment for MBC • Individualize treatment based on tumour burden and patient characteristics • Goals of treatment: • Prolong survival • Relieve symptoms with minimal treatment-related toxicities (integral part of overall care) • Discuss clinical trials when appropriate