Download
1 / 34
1.32k likes | 5.07k Vues
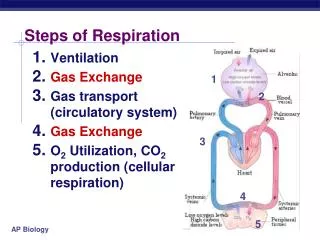
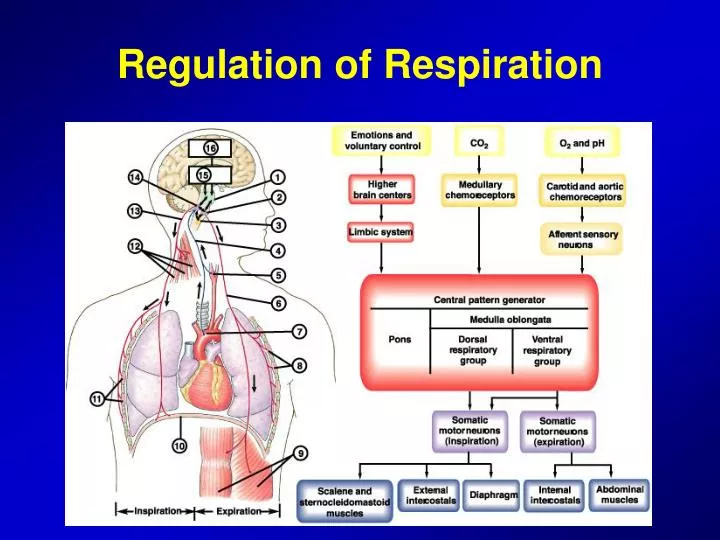
Regulation of Respiration. Respiratory Center. The respiratory center is composed of several groups of neurons located bilaterally in the medulla oblongata and pons of the brain stem 1) Dorsal respiratory group (respiration) 2) Ventral respiratory group (expiration)

E N D
Respiratory Center • The respiratory center is composed of several groups of neurons located bilaterally in the medulla oblongata and pons of the brain stem • 1) Dorsal respiratory group (respiration) • 2) Ventral respiratory group (expiration) • 3) Pneumotaxic center, which controls rate and depth of breathing • The dorsal respiratory group neurons play the most important role in the control of respiration
Dorsal Respiratory Group of Neurons • Its control of inspiration and of respiratory rhythm • Most of DRG neurons are located within the nucleus tractus solitarius • NTS is the sensory termination of both the vagal and the glossopharyngeal nerves which transmit sensory signals into the respiratory center from • Peripheral chemoreceptors • Baroreceptors • Several types of receptors in the lungs
Dorsal Respiratory Group of Neurons • Rhythmical inspiratory discharges from the dorsal respiratory group: basic rhythm of respiration is generated mainly in the dorsal respiratory group neurons • Inspiratory ramp signal: The nervous signal that is transmitted to the inspiratory muscles (mainly the diaphragm) is not an instantaneous burst of action • It begins weakly and increases steadily in a ramp manner for about 2 seconds • The advantage of the ramp is that it causes a steady increase in volume of lungs rather than inspiratory gasps
A pneumotaxic center limits the duration of inspiration and increases the respiratory rate • The pneumotaxic center transmits signals to the inspiratory area • It controls the “switch off” point of the inspiratory ramp • Strong or weak pneumotaxic signals and duration • It has a secondary effect of increasing the rate of breathing • Strong pneumotaxic signal and 30-40 breaths per minute • Or weak signal and 3-5 breaths per minute
Ventral Respiratory Group of Neurons • These neurons remain inactive during normal quiet respiration • Respiratory signals spill over into the ventral respiratory neurons from the dorsal respiratory area • Neurons in the VRG contribute both to inspiration and expiration • They are especially important in providing the powerful expiratory signals to the abdominal muscles during heavy expiration
Lung Inflation Signals Limit Inspiration • The Hering-Breuer Inflation Reflex: • Stretch receptors are located in the walls of bronchi and bronchioles throughout the lungs • They transmit signals through N Vagus into the DRG when the lungs are overstretched and switch off the inspiratory rump • It stops further inspiration • A protective mechanism for preventing excess lung infation, is not activated unless tidal volume is greater than 1500 ml
Chemical Control of Respiration • The ultimate goal of respiration is to maintain proper concentrations of O2, CO2 and H ions in the tissues • Excess CO2 and H ions in the blood mainly act on the respiratory center itself • O2 does not have a significant direct effect on the brain • Instead, it acts almost entirely on peripheral chemoreceptors in carotid and aortic bodies • These receptors transmit appropriate signals to the respiratory center of respiration
Direct Control by CO2 and Hydrogen Ions • Chemosensitive area of the respiratory center • Excitation of the chemosensitive neurons by H ions is likely the primary stimulus • Hydrogen ions do not easily cross the BBB • CO2 stimulates the chemosensitive area: • Although CO2 has little direct effect in stimulating the neurons, it does have a potent indirect effect • It reacts with H2O of the tissues and form H2CO3 • H2CO3 in turn dissociates into HCO3 and H ions
Central (medullary) Chemoreceptors (mechanisms) the H+ (CO2) sensors H+
Decreased Stimulatory Effect of CO2 After the First Days • Excitation of the respiratory center by CO2 is initially great • After 1 or 2 days, it gradually decreases • Part of this decline results from renal readjustment • HCO3 ions in blood diffuse through the BBB and combine with H ions • A change in CO2 therefore has a potent acute effect, but only a weak chronic effect after a few days’ adaptation
Quantitative effects of blood CO2 and H ion concentration on alveolar ventilation
Unimportance of Oxygen for Control of the Respiratory Center • Changes in O2 concentration have virtually no direct effect on the respiratory center • Hemoglobin-oxygen buffer system delivers normal amounts of O2 to tissues when pulmonary PO2 changes dramatically
Peripheral Chemoreceptor System • Carotid bodies: nerve fibers pass through Hering’s nerves to the N Glossopharyngeus • Aortic bodies: nerve fibers pass through the N Vagus • Both transmit to the dorsal medullary respiratory area
Peripheral Chemoreceptor System • Stimulation of chemoreceptors by decreased arterial O2 Effect of CO2 and H ions on chemoreceptor activity • Stimulation by way of peripheral chemoreceptors occurs as much as five times as rapidly as central stimulation
Effect of low arterial O2 to stimulate alveolar ventilation • When arterial CO2 and H ion level remain normal • Chronic breathing of low O2 stimulates respiration • This is called “acclimatization” • Loss of sensitivity to PCO2 after the first days • Low O2 can drive the respiratory system to a much higher level of alveolar ventilation than under acute conditions
Regulation of Respiration During Exercise • In strenuous exercise, O2 consumption and CO2 formation can increase as much as 20-fold • The arterial PO2, PCO2 and pH remain almost exactly normal • Then, what causes intense ventilation during exercise? • The brain, on transmitting motor impulses to the exercising muscles, transmits at the same time collateral impulses to the brain stem to excite the respiratory center • This is similar to stimulation of the vasomotor center during exercise that increases arterial pressure
Interrelations between chemical and nervous factors • At the onset of exercise, the alveolar ventilation increases instantaneously without an initial increase in arterial PCO2
Effect of maximum exercise to shift the alveolar PCO2-Ventilation response curve to a level much higher than normal
Other Factors That Affect Respiration • Voluntary control of respiration: hyper- or hypoventilation • Effect of irritant receptors in the airways: pulmonary irritant receptors, coughing and sneezing • Function of Lung “J receptors”: A few sensory nerve endings are located in the alveolar walls in juxtaposition to the capillaries – feeling of dyspnea • Effect of brain edema: Activity of the respiratory center may be depressed or even activated by brain edema • Edema can be relieved by using intravenous hypertonic solutions such as mannitol
Other Factors That Affect Respiration • Anaesthesia • Periodic breathing: an abnormality of respiration called periodic breathing occurs in a number of disease conditions • Cheyne-Stokes breathing
Sleep Apnea • Apnea means absence of spontaneous breathing • In sleep apnea, frequency and duration are greatly increased with episodes of apnea lasting for 10 sec or longer • Obstructive sleep apnea is caused by blockage of the upper airway • Muscles of the pharynx normally keep this passage open to allow air to flow into the lungs during inspiration • During sleep, these muscles usually relax, but the airway passage remains open enough to permit adequate air flow
Sleep Apnea • Clinical manifestatios: loud snoring and • labored breathing occur soon after falling asleep • Daytime drowsiness, Increased sympathetic activity • High heart rates, Pulmonary and systemic hypertension • and increased risk of developing CVD • Central sleep apnea occurs when the neural drive to respiratory muscle is transiently abolished • CNS drive to the ventilatory muscles may transiently cease • It may be caused by damage to the central respiratory center
Abnormal airway during sleep. Multiple sites of obstruction often occur in patients with obstructive sleep apnea. An elongated and enlarged soft palate impinges on the posterior airway at the level of the nasopharynx and oral pharynx. In addition, a retruding jaw pushes an enlarged tongue posteriorly to impinge on the hypopharyngeal space.
Anatomy of obstructive sleep apnoea.Coronal section of the head and neck showing the segment over which sleep related narrowing can occur (arrows).
Pathophysiology • Enlarged uvula resting on the base of the tongue (large arrow), along with hypertrophied tonsils (small arrows). The posterior pharyngeal erythema may be secondary to repeated trauma from snoring or gastroesophageal reflux
Treatment • The mechanism of action is due to the mechanical effects of raising the intraluminal upper airway pressure. • CPAP is applied with a nasal mask, nasal prongs or a mask that covers both the nose and the mouth.
Treatment • The rear portion of the soft palate and the uvula is removed. • The yellow portion is the one removed.
Normal Respiratory Rates • Infant 30-60 • Toddler 24-40 • Preschooler 22-34 • School-age child 18-30 • Adolescent 12-16 • Adult 10-20
Auscultation • 12 anterior locations • 14 posterior locations • Auscultate symmetrically • Should listen to at least 6 locations anteriorly and posteriorly