Download
1 / 43
470 likes | 795 Vues
Overview of Target-Specific Oral Anticoagulants (TSOACs). The Blood Thins and the Plot Thickens. American College of Physicians Annual Scientific Meeting November 7, 2014. Allison Burnett, PharmD, CACP, PhC Clinical Assistant Professor- UNM College of Rx

E N D
Overview of Target-Specific Oral Anticoagulants (TSOACs) The Blood Thins and the Plot Thickens American College of Physicians Annual Scientific Meeting November 7, 2014 Allison Burnett, PharmD, CACP, PhC Clinical Assistant Professor- UNM College of Rx Team Lead- Inpatient Anticoagulation Services University of New Mexico Hospital
Disclosures • Anticoagulation Forum • Board member • Honoraria • Society of Hospital Medicine (SHM) • Honoraria • Island Peer Review Organization (IPRO) • Honoraria
Case 1 Which of the following patients would be considered a good candidate for TSOAC therapy? A. 64-year-old male with a St. Jude’s mechanical mitral valve B. 65-year-old female with diabetes & hypertension (both well-controlled with medication), normal kidney function and new onset atrial fibrillation C. 37-year-old female with end-stage renal disease, on hemodialysis, who has thrombosed her dialysis fistula D. 54-year-old male with a history of recurrent VTE and labile INR due to non-compliance with warfarin therapy
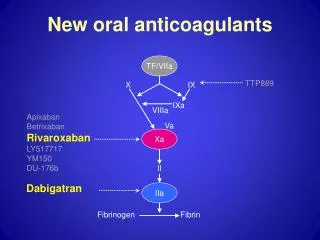
TSOAC: Mechanism of Action Adapted from Weitz JI, Bates SM. J ThrombHaemost 2005; 3: 1843-53.
TSOACs: Approved Indications Siegal DM, et al. J Thromb Thrombolysis 2013; 35: 391-98. ACS = acute coronary syndrome; NVAF = non-valvular atrial fibrillation; PPX = prophylaxis; TX = treatment; VTE = venous thromboembolism
Comparison of Oral Anticoagulants P-gp = p glycoprotein 3A4 = cytochrome P450 3A4 qual = qualitative Cove CL, Hylek EM. J Am Heart Assoc. 2013; 2:e000136.
TSOACs: Advantages • Improved pharmacokinetic/pharmacodynamic profile • Rapid onset/offset of action • Fewer dietary and drug interactions • Wide therapeutic window allows fixed dosing • No need for routine monitoring • Greater convenience and patient satisfaction • Improved safety profile • Potentially more cost-effective Bauer KA. ASH Education Book 2013; 1:464-470 Ruff CT, et al. Lancet 2013; 383 (9921): 955-62
TSOACs: Disadvantages • Dose reduction or avoidance in kidney impairment • Lack of flexibility in dosing • Short half-life mandates strict compliance • Limited availability of lab assays to measure anticoagulant effect • Lack of antidote • Higher drug acquisition costs • Fewer studied/approved indications (e.g., valves, ACS) Bauer KA. ASH Education Book 2013; 1:464-470 Majeed A, et al. Circulation 2013; 128)21): 2325-32
TSOAC: Dosing • Varies by: • TSOAC • Indication • Country • May require adjustment for: • Renal impairment • Age • Weight • Drug interactions • A combination of the above
TSOACs: Dosing (FDA Labeling) * Adjusted for renal impairment, drug interactions, age, low weight or a combination of these factors Treatment doses of rivaroxaban should be taken with largest meal of the day
Appropriate Patient Selection • No contraindication to TSOAC • e.g., pregnancy, mechanical valve • Good compliance history or highly likely to be compliant with medication and follow-up plan • Adequate organ function • Lack of significant drug-drug interactions with TSOACs (e.g. azoles, macrolides, antiepileptics, protease inhibitors, antacids, several cardiac medications) • Confirmed ability to obtain medication longitudinally Ageno W, et al. J ThrombHaemost 2013; 11: 177-9.
Case 2 A 46-year-old male on rivaroxaban x 2 weeks for acute PE presents to the ED with severe GI bleed.Labs and vitals: SCr2.3 mg/dL, Hgb/Hct4.2/12, BP 90/50, HR 120s. Which of the following labs would be most helpful in assessing for presence of rivaroxaban? A. Ecarin clotting time (ECT) B. Prothrombin time (PT) C. Activated partial thromboplastin time (aPTT) D. Thrombin time (TT)
Measurement of TSOACs • Increased specificity for target inhibition • Predictable pharmacokinetic and pharmacodynamic response • Minimal dietary effect • Less intrasubject and intersubject variability • Wide therapeutic index • Do not require routine monitoring • Dose is not adjusted based on laboratory measurements • No “therapeutic ranges” are provided
Measurement of TSOACs • When might measurement of a TSOAC be indicated? • Determine presence and quantity of drug • Urgent or emergent invasive procedure • Neuraxial anesthesia • Major trauma • Potential thrombolysis in acute thrombosis • Assessing compliance • Hemorrhagic or thrombotic complications • Assess drug accumulation • Diminished/changing renal function • Hepatic impairment • Accidental or intended overdose • Drug interactions Adcock DM. ASH Education Book 2012 ; 2012 (1): 460-65. Garcia D et al. J ThrombHaemost 2013; 11: 245-52. Tripodi A. Blood 2013; 121: 4032-35.
Measurement of TSOACs • Routine coagulation assays • Activated partial thromboplastin time (aPTT) • Prothrombin time (PT) • Helpful in determining relative drug concentration (qualitative) • Readily available in most reference labs • Specialty coagulation assays • Thrombin time (TT) • Dilute thrombin time (dTT) • Ecarin clotting time (ECT) • Chromogenic Anti-Xa • Determine measured drug concentration (quantitative) • Not readily available nor standardized • Research or investigational use only at this point
Effect of TSOAC on Coagulation Assays Measurement of TSOACs *Variability by reagent/instrumentation **Drug-specific TT = thrombin time ECT = ecarin clotting time Hillarp AJ, ThrombHaemost 2011;9:133-9. Funk DM, Hematology 2012:460-465. Frost et al, Br J ClinPharmacol 2012;75:476. Garcia D, et al. J ThrombHaemost 2013; 11: 245-52.
Measurement of TSOACs “Rules of Thumb”
Case 3 A 62-year-old male with atrial fibrillation (CHADS2score of 2 for DM, HTN) on a TSOAC for stroke prevention is scheduled to undergo total knee replacement in a few weeks. Labs: SCr 0.7 mg/dL, weight 83 kg, Hgb 10.2, Hct31 Which of the following describes the best course of action for his peri-procedural anticoagulation? A. Do not interrupt TSOAC therapy for this procedure B. Hold TSOAC for 2-3 half-lives prior to this low bleed risk procedure C. Hold TSOAC for 4-5 half-lives prior to this high bleed risk procedure D. Hold TSOAC for 5 days prior to procedure and use LMWH as bridging therapy
Peri-Procedural Management: TSOACs • ~250,000 patients annually in the US evaluated for anticoagulation management around elective procedures • Rapid onset/offset of TSOACs precludes need for peri-operative bridging with heparin or LMWH • Key question: Does anticoagulation need to be interrupted? • Timing of cessation and resumption of TSOAC is based on: • Patient’s renal function • Half-life of TSOAC • Type of procedure and anesthesia SpyropolousAC, et al. Blood 2012; 120(15): 2954-62.
Assessing Thrombotic Risk Spyropolous AC, et al. Blood 2012; 120(15): 2954-62
Assessing Bleed Risk Baron TH, et al. N Engl J Med 2013; 368: 2113-24.
Peri-Procedural Management: TSOACs • Management of Anticoagulation in the Peri-procedural Period (MAP) Tool • Available at http://qio.ipro.org/drug-safety/drug-safety-resources or http://excellence.acforum.org/
Peri-Procedural Management: TSOACs • Cessation of TSOAC • Dependent on patient’s renal function and half-life of TSOAC • Half-life ranges from 6-17 hours, depending on TSOAC • Will be prolonged with renal impairment • May almost double in severe impairment • May require longer pre-op hold time • Dependent on type of procedure • Low bleed risk: hold for 2-3 half-lives • High bleed risk: hold for 4-5 half lives Stangier J, et al. ClinPharmacokinet 2010; 49(4): 259-68. Spyropolous AC, et al. Blood 2012; 120(15): 2954-62.
Peri-Procedural Management: TSOACs • Resumption of TSOAC • TSOACs have rapid onset of anticoagulant effect (~1-4 hours) • Analogous to using LMWH • Caution with resuming too soon or too aggressively • Timing of resumption dependent on type of procedure • Low bleed risk: resume 24 hours post-op • High bleed risk: resume 48-72 hours post-op • May consider “step-up” approach • Lower or prophylactic dose of TSOAC for initial 24-48 hours • If tolerated, increase to treatment dose TSOAC at 48-72 hours Spyropolous AC, et al. Blood 2012; 120(15): 2954-62.
Peri-Procedural Challenges • May need to confirm absence of anticoagulant effect • Emergent procedures • Planned use of spinal or epidural anesthesia • Ensure use of appropriate lab parameter • Delayed resumption of TSOAC • Patient unable to take PO post-procedure • Concern for impaired gastrointestinal absorption (e.g., post-op ileus) • Epidural or spinal anesthesia • Consider use of parenteral anticoagulant until patient can be appropriately switched to TSOAC Spyropolous AC, et al. Blood 2012; 120(15): 2954-62.
Case 4 A 71-year-old female on dabigatran for NVAF (CHA2DS2VASc = 6) and recurrent VTE was admitted for ACS and emergently taken to the cath lab for percutaneous coronary intervention (PCI). She was found to have multi-vessel disease and had 2 drug-eluting stents placed, which will require dual antiplatelet therapy. Which of the following antithrombotic strategies would be the best option for her? A. Resume dabigatran along with dual antiplatelet therapy indefinitely B. Stop dabigatran. Overlap LMWH and warfarin until INR >2, along with antiplatelet therapy D. Stop anticoagulation and continue only dual antiplatelet therapy
Switching Between Anticoagulants • Reason for switching from parenteral to oral anticoagulant • Facilitate longer-term outpatient management • Reasons for switching from warfarin to TSOAC • Drug intolerance • Therapeutic failure • Patient preference • Reasons for switching from TSOAC to warfarin • Drug intolerance • Therapeutic failure • Patient preference • New comorbidity or contraindication • Worsening renal function • Mechanical heart valve • Acute coronary syndrome (ACS) requiring dual antiplatelet therapy Abo-Salem E, et al. J Thromb Thrombolysis 2014; 37: 372-79.
Switching Between Anticoagulants • Can place patients at undue risk for adverse events • e.g., bleeding or thrombosis • Requires a “carefully constructed and thoughtful approach” • Should be based on: • Pharmacokinetic profile of each anticoagulant • Appropriate laboratory assessment of patient’s coagulation status • Patient’s renal function Abo-Salem E, et al. J Thromb Thrombolysis 2014; 37: 372-79.
Switching Between Anticoagulants • Unfractionated heparin • Short half-life precludes need for lag time until alternative anticoagulant is initiated • TSOACs and SQ injectables (LMWH, fondaparinux) • Longer half-life requires lag time until alternative anticoagulant is initiated • Start alternative anticoagulant when the next dose of original anticoagulant would be due • Warfarin • Extremely long half-life requires confirmed offset via INR • Slow onset may require overlap of rapid-acting anticoagulant
Case 5 A 62-year-old female on apixaban 2.5 mg PO BID for VTE prophylaxis after a total hip arthroplasty presents to the ED with mild hematuria. She is hemodynamically stable. When asked, she states she last took her apixaban yesterday morning, and missed her evening dose due to not feeling well. What are options for managing her bleeding episode? A. Hemodialysis to remove the apixaban B. Oral activated charcoal to remove the apixaban C. Concentrated factors (PCC, aPCC, rFVIIa) to reverse apixaban D. Supportive care and investigate for source of the bleed
Management of Severe Bleeding: TSOACs • General approaches • Hold anticoagulation • Determine time of last ingestion • Tincture of time (short half-lives) • Fluid resuscitation to promote renal excretion • Transfusion of blood products • Attempt to identify and address source of bleed • Mechanical compression • Have specialty services on standby • If inadequate response, consider reversal strategies
Hierarchy of Evidence: Reversal of TSOACs Seigal DM, Cuker A. Drug Discov Today 2014. [Epub ahead of print] PMID: 24880102.
Concentrated Factors for TSOAC Reversal • Clinical outcome data on the efficacy of PCC, aPCCand rFVIIa for the reversal of TSOACs are lacking • Available evidence is limited (healthy human volunteers, animal models, in vitro studies) with conflicting results • These agents may be considered in addition to maximum supportive measures in patients with severe/life-threatening bleeding • The net clinical benefit should be considered in light of their prothrombotic potential (~ 1.4% for PCC; up to 10% with rFVIIa) • Specific reversal agents are in development Dentali F. ThrombHaemost. 2011 Sep;106(3):429-38. PMID: 21800002. Levi M. N Engl J Med. 2010 Nov 4;363(19):1791-800. PMID: 21047223. Seigal DM, Cuker A. Drug Discov Today 2014. [Epub ahead of print] PMID: 24880102.
Management of Severe Bleeding: TSOACs Kaatz S. Am J Hematol. 2012 May;87 Suppl 1:S141-5. PMID: 22473649.
Summary • TSOACs may provide a viable alternative to traditional anticoagulants in appropriately selected patients • Optimal use of TSOACs requires familiarity with: • Pharmacokinetic/ pharmacodynamic profiles • Various dosing strategies • Laboratory measurement • Peri-procedural strategies • Switching strategies • General approaches to bleed management • Familiarity with reversal strategies