Download
1 / 12
120 likes | 527 Vues
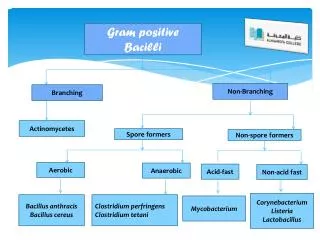
Outbreak of Gram Positive Bacterial Keratitis Associated with Epidemic Keratoconjunctivitis in Neonates and Infants. Joo Hoon Kim 1 , Mee Kum Kim 1 , Joo Youn Oh 1 , Ki Cheol Jang 1 , Won Ryang Wee 1 , Jin Hak Lee 2

E N D
Outbreak of Gram Positive Bacterial Keratitis Associated with Epidemic Keratoconjunctivitis in Neonates and Infants Joo Hoon Kim1, Mee Kum Kim1, Joo Youn Oh1, Ki Cheol Jang1, Won Ryang Wee1, Jin Hak Lee2 Department of Ophthalmology, Seoul National University College of Medicine, Seoul, Korea1 Department of Ophthalmology, Seoul National University Bundang Hospital, Seongnam, Gyeonggi-do, Korea2 *All authors in this study declare no financial interest.
The outbreak of Epidemic Keratoconjunctivitis(EKC) • In a community, yearly • In a health care unit (HCU), not uncommon • Neonatal intensive care unit (workers, patients) • Nursing home • The outbreak of EKC in NICU at SNUH in 2007 • There is only 1 case of bacterial keratitis after EKC • Alcaligenes Xylosoxidans (gram-negative rod) • Oh et al. Korean J Ophthalmol. 2005 Sep;19(3)
Purpose To report the clinical characteristics of bacterial keratitis associated with outbreak of EKC To evaluate the risk factors for the development of bacterial keratitis in eyes with EKC Design • Retrospective case-control study with hospital based case series Participants • 108 patients (45 adults and 63 children) diagnosed as EKC in a tertiary eye-care center from July 2007 to August 2007 • 9 out of 108 patients who were treated with bacterial keratitis after an episode of EKC
Methods (1) Clinical aspects of bacterial keratitis after EKC • Demographic data: sex, age at infection, HCU-association • Microbiological profile, onset of keratitis after EKC, corneal findings and classification • Treatment outcome (2) Risk factors assessment for bacterial keratitis • Definition • Bacterial keratitis: Any Infective corneal lesion with bacterial corneal cultures (+) or conjunctival bacterial swap culture (+) • EKC:Clinical signs (follicular hypertrophy, exudative membrane, lacrimal swelling, mucoid discharge, redness and no other identified cause of conjunctivitis) and if possible, (+) result of Adenovirus Immunofluoresence assay (IFA) or culture • Risk factors (statistical analysis) • Use of steroidat early EKC period (Fisher’s test) • Interval of F/Uat early EKC period (Mann-Whitney test) • MRSA colonization in conjunctiva and other part of body (Fisher’s test) • Gestational age (Mann-Whitney test) • Body Weight at infection (Mann-Whitney test) • Duration of hospitalization(Mann-Whitney test)
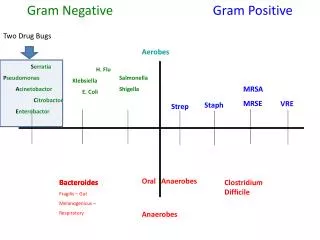
Result • Epidemiology of EKC, Bacterial keratitis and Microbiological Features • The incidence of bacterial keratitis(Table 1) • Most bacterial keratitis(88%): neonates and infants • Significantly higher in HCU-based inpatients or childrencompared with population-based patients or adults • Causative organism of bacterial keratitis(Table 2) • Methicilline resistant Staphylococcus aureus(MRSA) • Most frequently found (7 cases) • Coinfected with Staphylococcus epidermidis and Pseudomonas aeruginosa (1 case) • Streptococcus pyogenes (1case)
Principle treatment of keratitis • Onset of ketatitis after EKC (Table 2) • Mean: 8.8 days (3-12days) • Treatment • Initial Tx at EKC • Topical ecolicin with or without topical steroid • Initial Tx at Keratitis • Discontinuation of steroid • Systemic antibiotics: IV Vancomycin, Amikin • Local treatment • 3.1 % Vancomycin sol. q 1hr, 2% Amikin sol. q 1hr • Change according to the reported sensitivity test • If unresponsive to treatment • 5% T-vanco ointment 6/d, 0.5% moxifloxacin sol. q 2hr • Surgical treatment : 1 case (due to impending perforation) (Fig 1E) • Amniotic membrane transplantation (Fig 1F, G, H)
Clinical manifestation of bacterial keratitis and Outcome of treatment (Table 2) • Shallow infiltrations with epithelial defect (n=2) (Fig.1A) • Mean healing time: 9±5.6 days (range: 5-13 days) • Corneal sequels after 3 mo: (-) • Stromal infiltrates underlying epithelial defects (n=7)(Fig.1B, C) • Mean healing time: 25.6±16.7 days (range: 10-51 days) • Corneal sequels after 3 mo • Diffuse stromal new vessle: 83.3%(5/6) • Corneal opacity: 67.7%(4/6) (Fig 1D) • Though bacterial keratitis had been resolved in all of the patients, 44.4% (4/9) of bacterial keratitis patients have been requiring corneal transplantation due to dense central opacity (3 months follow-up)
Risk factors assessment for bacterial keratitis • Incidence of bacterial keratitis • Significantly higher in HCU stayed patients and children (especially in neonate and infants)(Table 1) • Using topical steroid in early EKC • Not significantly different in HCU-based (30%:16/54) and population-based (46%:25/54) EKC patients (p=0.07, χ2 test) • In the HCU stayed children • Factors significantly higher in bacterial keratitis group • Culture positive rate of MRSA in conjunctiva (Table 3) • Incidence of using topical steroid in early EKC period (Table 3) • Longer interval of follow-up examinations in early EKC period (Table 4) • Factors with no differencebetween bacterial keratitis and EKC group (Table 4) • (+) Results for either adenoviral IFA or culture • MRSA colonization of other parts of body • Gestational age • Duration of hospitalization
Conclusion • Infants including neonates show high tendency of MRSA keratitis accompanied with EKC, especially in HCU stayed inpatients • MRSAcolonization in conjunctiva, use of topical steroid and longer interval of follow-up for EKC can be a risk factor in development of MRSA keratitis
Discussion • Why bacterial keratitis after EKC in neonate and young infant? • Weak physical barrier in the premature1 • epidermal barrier: mature around the 32nd or 34th week of gestation • Weak mucosal membrane immunity2 • lower the sIgA in preterm infants at the age of 3 to 8 postnatal months • Weak innate and specific immunity to pathogen2 • Unable to complain EKC destruction of corneal integrity &Compromised surface Highly susceptible of infection
MRSA infection3 • 12%: community-associated, 85%: health care-associated • MRSA nares colonization4 • MRSA colonization in nares: 25% of MRSA infection rate compared with 2.0% of the uncolonized • MRSA ocular surface colonization and nasalcarriage5 • Conjunctival MRSA (+) : Anterior nares of MRSA 78% • Conjunctival MRSA (-) : Anterior nares of MRSA 11% • SNUH NICU6 • 10.4%:neonates became colonized for MRSA in nasal/ inguinal cultures • The mean time to acquire MRSA colonization was 17.1 days (1-471days) • WhyMRSAkeratitis inhealthcare unit? Compromised surface with EKC may elicit MRSA keratitis!! Risk factor: MRSA colonization, Topical steroid use, Long interval of F/U
References 1. Cartlidge P. The epidermal barrier. Semin Neonatol. 2000;5:273-80. 2. Adkins B, Leclerc C, Marshall-Clarke S. Neonatal adaptive immunity comes of age. Nat Rev Immunol 2004;4:553-64. 3. Naimi TS, LeDell KH, Como-Sabetti K et al. Comparison of community- and health care-associated methicillin-resistant Staphylococcus aureus infection. JAMA 2003;290:2976-84. 4. Davis KA, Stewart JJ, Crouch HK et al. Methicillin-resistant staphylococcus aureus (MRSA) nares colonization at hospital admission and its effect on subsequent MRSA Infection. Clin Infect Dis. 2004;39:776-82. 5. Kimura N, Sotozono C, Higashihara H et al. Relationship between ocular surface infection or colonization of methicillin-resistant Staphylococcus aureus and nasal carriage. Nippon Ganka Gakkai Zasshi. 2007;111:504-8. 6. Kim YH, Chang SS, Kim YS et al. Clinical outcomes in methicillin-resistant Staphylococcus aureus-colonized neonates in the neonatal intensive care unit. Neonatology 2007;91:241-7.