Download
1 / 16
180 likes | 399 Vues
Pathophysiology of myocardial ischaemia and Acute Coronary Syndromes (ACS). Rick Allen. Acute coronary syndromes include: Unstable angina Acute myocardial infarction Sudden cardiac death Basics of pathophysiology Stable atherosclerotic plaque unstable atherothrombotic lesion

E N D
Pathophysiology of myocardial ischaemia and Acute Coronary Syndromes (ACS) Rick Allen
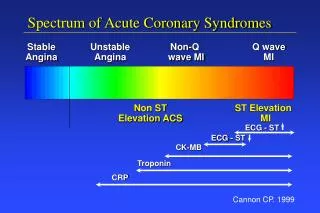
Acute coronary syndromes include: • Unstable angina • Acute myocardial infarction • Sudden cardiac death • Basics of pathophysiology • Stable atherosclerotic plaque unstable atherothrombotic lesion • Rupture, superficial erosion deep haemorrhage, ulceration, fissuring. • Change results in the formation of a thrombis which causes partial or complete occlusion of the vessel
Angina • Stable • ↑ myocardial O2 demand > ability of stenosed coronary art. to deliver. • Due to ↑ physical activity, emotional excitement or ↑ workload. • Prinzmetal • Caused by vasospasm. May be no/minor athersclerotic presence • Unstable • plaque rupture partially occlusive thrombosis + vasoconstriction severe but transient ↓ in coronary blood flow. • Thromboembolican micro infarcts. • Occurs with low exercise or at rest.
Angina • The ischaemic episode can last from 15s up to 15 minutes, meaning that no (/minimal?) myocyte necrosis occurs.
Myocardial Infarction • Acute plaque change • platelet adherence to exposed collagen/necrotic plaque contents, combine to form microthrombi • platelets release mediators causing vasospasm • TF release act. Coagulation cascade, ↑ thrombus • occludes lumen.
Myocardial Infarction • Other causes • Vasospasm : platelet loitering or cocaine use • Emboli: from LA due to AF, left sided mural thrombosis, infective endocarditisvegitation, right sided source via patent foramen ovale • Low systemic BP: e.g. shock, ↓ perfusion • Vasculitis, vascular dissection • Haematological issues like sickle cell causing occlusion
Myocardial Infarction • Reversible: • Aerobic metabolism stops no ATP production and accumulation of toxic metabolites (lactic acid) • Loss of contractility in 60 secs. This can cause death prior to the production of an infarct. • Irreversible: • Leaky cell membrane intracellular components leak into cardiac interstitium microvasculature and lymph. • >1hr, damage to microvasculature • Permanent myocardium damage 2 - 4hrs.
Progression of Infarct • Begins as subendocardial (dependent on cause) and then moves as a wavefront transmurally • The inner 1/3 is the least perfused region and is therefore the most susceptible. • Regionally isolated if thrombus is lysed early • Circumferential in prolonged, severe ↓ systemic BP (shock + non-critical stenosis) • Transmural infarct gives ST elevation, subendcardial does not
Factors Determining Morphology • Location, severity, rate of development of coronary obstructions • Size of vascular bed perfused by occluded artery • Duration of occlusion • Metabolic/O2 needs of myocardium at risk. • Collateral vessels • Presence, site, severity of vascular spasm • HR, rhythm, blood oxygenation. • **Necrosis is complete in 6hrs, longer if collaterals are present**
Sudden Cardiac Death • atherosclerotic lesion disrupted plaque regional myocardial ischaemia fatal ventricular arrythmia • Can be the first clinical presentation of IHD • AMI is the most common trigger for fatal arrhythmias (e.g. VF, asystole) • Injury can affect the conduction system and create electrochemical cardiac instability. • Fatal arrhythmias are usually caused by electrical instability distant from the conduction system – arrythmogenic foci are often located adjacent to scars of old MI’s.
Non-atherosclerotic causes include • Pulmonary HTN • Congenital abnormalities • Aortic valve stenosis • Mitral valve prolapsed • Myocarditis • Dilated or hypertrophic cardiomyopathy • Cardiac hypertrophy • Genetic (channel or proteins which assist the channels functioning are faulty, often leading to long QT intervals.)
Dilation of Ventricles • Dilated cardiomyopathy • Genetic • Myocarditis (sometimes due to viruses) • Alcohol and other toxins • Childbirth (↑ volume?) • Ventricular remodelling • Response to injury or changes in loading • Adaptive
References • Robbins and Cotran