Download
1 / 48
480 likes | 643 Vues
Natural Delivery, Family Practice Style. Samantha Maplethorpe, M.D., M.P.H. Goals. Improve knowledge and confidence in management of childbirth among Family Practice residents Enhance advancement through different developmental stages during maternity care training in residency.

E N D
Natural Delivery,Family Practice Style Samantha Maplethorpe, M.D., M.P.H.
Goals • Improve knowledge and confidence in management of childbirth among Family Practice residents • Enhance advancement through different developmental stages during maternity care training in residency
Training Level Specific Stages As of June: • R1s: Begin continuity patient deliveries, function more autonomously, gain comfort in prenatal care and counseling • R2s: Develop own style, increase decision making capacity, increase independence, build confidence in decisions • R3s: Prepare to fly solo, work in different hospitals, and with different populations
Questions for the Audience • What is Natural Delivery? • What defines transition? • Does water immersion increase chance for infection? • Does labor induction increase C-sections? • What would you say if your patient asked you to attend her for home birth? • Childbirth Classes: Advise attendance?
Objectives By the end of this talk, you will be able to: • Define “Natural Delivery” • Describe the unique approach of Family Centered Maternity Care • Identify resources on evidence-based maternity care • Discuss the evidence supporting various interventions and non-interventions in labor and delivery
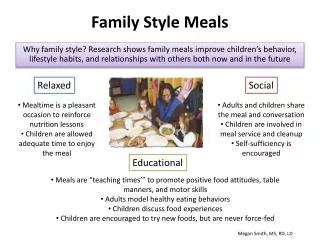
Family Centered Maternity Care Seeking care that is the “best of all worlds” Why do we do what we do so well? • Patient-Centered • Evidence Based • Community-Oriented
Definitions • Natural Delivery • Patient-Centered Care • Evidence-Based Practice • Community-Oriented
Definitions: Natural Delivery • What does “Natural Delivery” mean? • No epidural? • No pain meds? • Place of birth? At home? • No interventions such as IVs, amniotomy, IUPC, FSE, EFM? • Hands on vs. hands poised?
Definitions: Natural Delivery (cont.) • “Primum non nocere” • Informed by knowledge of and respect for normal labor physiology • Emphasizes working in tune with natural processes • Respects the mother-baby dyad
Definitions: Natural Delivery (cont.) • Approaches labor management as a continuum with pregnancy and new parenthood • Builds on prenatal rapport with parents and subsequent care for newborn • Treats labor & delivery as a “family” experience • Interventions performed only when evidence supports their use for specific maternal or fetal indications.
Definitions: Patient-Centered • Build doctor-patient relationship over the course of prenatal care, which allows for longitudinal discussion & patient education • Listen to patient’s & family’s wishes, ideas • Negotiate goals with patient & family • Communicate openly to facilitate flexibility when changes changes in labor care necessary
Definitions: Patient-Centered (cont.) • Respect that this is the patient’s delivery • Recognize patients likely to have the most severe pain of their life (80% rated pain of labor “very severe” or “intolerable”) • Understand that pain varies among women, & each labor of an individual woman may be quite different • Take time to understand their perspective, past labor experiences, expectations.
Definitions: Evidence-based • Conscientious, judicious, and explicit use of current best evidence in making decisions about the care of individual patients • Counter to the tradition-based obstetric legacy
Definitions: Evidence-based (cont.) • Evidence in obstetrics? Archie Cochrane, 1972: • RCTs needed to better inform practices regarding pregnancy and childbirth • Obstetrics had been least successful in using research evidence to guide practice This approach & concern expanded to all other areas of medicine Systematic reviews of RCTs followed, and EBM was born
Reviewing the Evidence:Available Resources • American Journal of Obstetrics and Gynecology • Evidence-based Obstetrics & Gynecology • Maternity Center Association website • Clinical Evidence by BMJ • Cochrane Library • National Guideline Clearinghouse • Up To Date
Reviewing the Evidence:Assessing the Quality • Who does the studies, & how does this affect the questions that get asked? • Specialty-specific goals of care: -Priority given to each woman’s personal experience of childbirth -- sacrifice safety? -Minimize perinatal morbidity & mortality--increase mother’s risk or discomfort? -Rising cost of care & limited resources --decreases individual choice and sense of excellence?
Reviewing the Evidence:Assessing the Quality (cont.) • Differences in objectives result in different outcomes being measured, such as women’s satisfaction with childbirth or direct measures of death, disease, & disability, vs indirect measures of fetal well-being • Family Practitioners strive to balance these priorities, must be familiar with the evidence supporting decisions
Definitions: Community-Oriented • Tailor care to available treatments • Know available services: H20 immersion, “walking epidurals”, continuous care • Know standards of care in community • Know about community served: urban vs. rural, high risk vs. low risk, etc. • Consider societal imperatives: limited resources, patient safety, access, quality
Antepartum: Anticipation of Childbirth • Childbirth classes -- advise attendance? • Continuity of caregiver • GBS culture • Birth plans & expectations: - Preparing a hospital bag - Discussing labor events - Alleviating fears
Antepartum: Continuity of Care • Care during pregnancy, childbirth, and postnatal period often provided by multiple caregivers • Controlled trials comparing continuity of care with usual care during pregnancy, childbirth and the postnatal period • Studies show beneficial effects, but not clear whether these are due to greater continuity of care or to midwifery care.
Peripartum: Diagnosis of Labor • When should women call or come in? • Best times to come to hospital, avoid early admissions, improve outcomes • Avoiding early admissions leads to less anesthesia, fewer dystocias, fewer c-sections & better patient satisfaction
Peripartum: Induction of Labor • Prevention of post-dates • Stripping membranes • Breast stimulation • Okay to induce at 41 weeks with favorable cervix in a multip -- no increased risk of C-section
Peripartum: Other Interventions • Pubic or perineal shaving: no decrease in rates of infection, possible increase in rates of gram-negative infections • Enemas: no decrease in rates of infection or perineal complications, cause discomfort for women and increase costs of delivery
Peripartum: Other Interventions (cont.) • Continuous caregiver support: appears to have a number of benefits for mothers and their babies with no apparent harmful effects. • Hands-knees position for fetal malpresentation: appears to result in short term effects on fetal position; no other outcomes reported.
Intrapartum: Pain Management Pharmacologic: • Epidurals: superior pain relief; combination of anesthetics and opioids work best to block somatic component • Spinals: intrathecal analgesia w/opioids only allows for ambulation (doesn’t affect muscle strength)
Intrapartum: Pain Management (cont.) Pharmacologic (cont.): • Paracervical & pudendal blocks • Systemics: opioids, phenothiazines, antihistamines, barbiturates, benzodiazepenes, nitrous oxide, PCA’s
Intrapartum: Pain Management (cont.) Non-pharmacologic: • Transcutaneous electrical nerve stimulation (TENS): involves delivery of current through a series of electrodes applied to the skin surface; review of studies found it to be ineffective. • Hypnosis & acupuncture: not shown to be effective in studies, may work for individual women
Intrapartum: Pain Management (cont.) Non-pharmacologic (cont.) • Water immersion:No significant differences for pain relief, augmentation and duration of first stage of labour, meconium stained fluid and perineal trauma; neonatal outcomes such as Apgar scores, umbilical arterial pH values and neonatal infection rates also showed no differences.
Intrapartum: Pain Management (cont.) Non-pharmacologic (cont.) • Psychoprophylaxis: Emphasize patient’s role in controlling her own experience while receiving support from family and friends. • Little evidence that psychoprophylaxis, relaxation techniques, or even childbirth classes reduce psychological stress or increase satisfaction during labor.
Intrapartum: Pushing • Anatomical onset of 2nd stage may not coincide with expulsion phase & woman’s urge to bear down • If wants to push before 8 cm, needs methods to resist (panting, breathing techniques, pain relief • If a rim of cervix and urge to push, probably okay to do, but not to exhaustion • Epidurals may decrease, delay or increase urge to push
Intrapartum: Pushing (cont.) • “Laboring down” • Sustained breathholding and directed pushing may shorten 2nd stage of labor, but can decrease umbilical artery pH
Intrapartum: Positions • Upright posture vs. recumbent • Birth chair or stool: reduces episiotomies but increasd second degree tears and EBL perhaps due to trauma • Birth cushion/wedge: led to reduced 2nd degree tears, assisted deliveries while episiotomies and PPH were similar • Squatting position fine if woman is comfortable • Toilet for laboring down • Ultimately women should be encouraged to deliver in most comforatble position
Intrapartum: Duration of 2nd Stage • Widespread policy to impose arbitrary limits on 2nd stage based on nullip/multip status. • Associations but not causations have been made between longer second stage and perinatal mortality, PPH, puerperal fever, neonatal seizures, and acid-base status of baby.
Intrapartum: Duration of 2nd Stage (cont.) • Length of second stage is often curtailed by active pushing or operative delivery but maternal and fetal trauma may not be justified. • If mother and baby are stable, and there is evidence of descent there are no grounds for intervention.
Intrapartum: Perineal Care • Two-thirds of all nulliparous women sustain trauma requiring suture. • Vacuum should be used for maternal or fetal indications rather than forceps to reduce perineal trauma • Routine episiotomy not supported by the evidence • Type of suture material for repairs, continuous vs. interrupted stitches
Third Stage: Active versus expectant management • Evidence supports active management (pitocin, early cord clamping/cutting, controlled cord traction)
Early Skin to Skin Contact • Positive effects on breastfeeding, infant temperature, infant blood glucose, infant crying, maternal affectionate love/touch. • Breastfeeding within 30 minutes increases oxytocin to improve uterine contraction, placenta and blood expulsion.
Ongoing Evidence Based Reviews • Repair vs nonrepair of perineal trauma • Postnatal parental education for improving family health • Maternal positions and mobility during first stage labour • Restricting oral fluid and food intake during labour • Pushing/bearing down methods used during the second stage of labor
Case: Anxious Annie • 24 yo G1 at 20 weeks is looking forward to the birth of her first child and wants to know if she should prepare in any way. What do you tell her?
Case • Now at 37 weeks, uncomplicated pregnancy, has heard that pregnancy sometimes goes beyond her due date. She has carefully planned her relatives arriving and her maternity leave and wants to know what she can do to prevent being pregnant much past her due date. • What do you tell her? • What can you do? • Should she try primrose oil?
Case • She follows your advice and presents to L& D at 38 5/7 wks with her birth plan in hand and is ready for an epidural. Her cervix is 2 cm dilated, she has been contracting every 5 minutes for 3 hours. • What do you tell her? • What are the risks and benefits of an epidural, when can she get one, when is too late to get one?
Case: • She returns from walking 3 hours with her husband on L&D and is now at 4 cm dilation and has thought about that epidural and wants to wait for now. She is excited but a little scared and wants to hear more about pain management options at this point and techniques to help her baby come faster. • What would you like to tell her? • What would you like the L& D nurse to have available • The nurse would like to place an IV now, what do you say? • Annie wants to know if she can try the jacuzzi and can she have a little something to eat or drink?…is that okay?
Case • She has done well with positioning techniques, the labor ball and counterpressure but she is having a lot of back pain. You check her cervix and decide she is OP, what would you like to do? • Does she have to have these uncomfortable bands around her stomach all the time?
Case • After 2 more hours she is completely dilated and is in a lot of pain now, what do you say? • Should she start pushing? • Her husband isn’t sure what to do to help, any tips for him?
Case • She has been laboring down for two hours making slow but steady progress with adequate contractions and reassuring FHR tracing intermittently, she feels the urge to push, how long will you let her push before you intervene? • How will you guide her pushing? • What position should she be in? • Will you use techniques to massage the perineum while she pushes?
Case • She has pushed the baby downed and is crowning but the baby’s head doesn’t stay down between contractions, she is getting tired, any suggestions? • How will you manage her perineum during delivery of the head?
Case • With the use of the mirror she has successfully delivered the baby’s head, anterior and posterior shoulders follow easily, you clamp the cord and dad cuts the cord. No meconium, baby is pink and vigorous, what do you do with baby? • She has only a small midline posterior lac that looks like it could use a repair, what kind of suture would like to use, what will be your technique?
Case • Nice Job! You take numerous pictures with the family, help mom to get baby latched, finish paperwork in the room while answering questions and after about a half an hour you do the newborn exam with mom and dad and they thank you profusely.