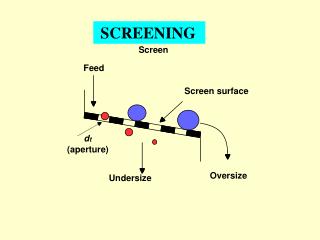
Screening
Screening. Phil Thirkell. What is screening?. A process of identifying apparently healthy people who may be at risk of a disease or condition Identify Apparently healthy Increased risk of a disease/condition. Give 4 screening programmes undertaken in the UK. Antenatal screening

Screening
E N D
Presentation Transcript
Screening Phil Thirkell
What is screening? • A process of identifying apparently healthy people who may be at risk of a disease or condition • Identify • Apparently healthy • Increased risk of a disease/condition
Give 4 screening programmes undertaken in the UK. • Antenatal screening • Postnatal screening – hearing, heel prick, neuroblastoma • Cervical smear • Mammography • Chlamydia screening • Bowel Cancer – FOBT • Prostate cancer • Abdominal Aortic Aneurysm • Depression – PHQ-9 questionnaire • etc.
Criteria for a Screening Programme • Wilson + Jungner criteria • Important health problem • Treatment available • Facilities available for diagnosis and treatment • Latent stage of the condition • Test available to detect the condition • Test is acceptable to the population • Natural history of the disease is known • Policy of who gets treatment has been made • Financially viable • Case-finding is a continual process, not just a one off
Neonatal screening • Which conditions are screened for with blood spot testing? • Phenylketonuria • Sickle cell disease • Cystic fibrosis • Congenital hypothyroidism • Medium-chain acyl-CoA dehydrogenase deficiency
Antenatal Screening • What is a pregnant woman screened for? • Pre-eclampsia • Rhesus antigen status / blood group • Anaemia • Diabetes • Syphilis • Hepatitis B/C • HIV
Anomaly Scan – USS between 18-21 weeks • What is an anomaly scan used for? • Spina bifida • Down’s syndrome • Hydrocephalus • Cleft lip/palate • Date the pregnancy • Sex of the baby • Multiple pregnancy • Organ development • Abdominal wall
Sensitivity • The number of people who have the disease who get a positive test result • True positive / (True positive + False Negative) • e.g. 50 people with known Rheumatoid Arthritis. RhF blood test is positive in 42 of the patients. • Sensitivity is 84%
Specificity • The number of people who don’t have a disease who are correctly told they don’t have it • True negatives / (True negatives + False positives) • E.g. 30 patients with no evidence of rheumatoid arthritis have a blood test for RhF. 2 patients have a positive result. • Specificity = 93%
Positive Predictive Value • The number of people who have a positive test result who actually do have the disease • True positives / (True positives/False positives) • e.g. 2500 PSA blood tests performed on men >65yr. 800 are raised above normal levels. Biopsy reveals that 95 of these have prostate cancer. • PPV = 95/(95+800) = 11%
Negative Predictive Value • The number of people who have a negative test result who definitely don’t have the disease • True negatives / (true negatives + false negatives) • e.g. 2500 PSA blood tests on men >65yrs. 1700 have normal PSA results. 20 of these turn out to currently have prostate cancer despite a normal PSA. • 1680/ (20 + 1680) = 98.8%
Screening Bias • Healthy screenee • Length time • Lead time • Overdiagosis
Healthy screenee • Proactive patients who turn up to screening opportunities take better care of themselves are less likely to have a positive result • Less likely to smoke, drink too much, have low income • More likely to exercise, eat healthily, attend healthcare at other times • Internal locus of control
Length time • Screening appears to improve prognosis because slow-forming conditions are detected and treated earlier than they would compared to waiting for symptoms to start • e.g. 500 slow forming and 500 fast forming cancers happen each year • Slow forming – no symptoms and better prognosis • Fast forming – obvious symptoms and poor prognosis • Screening can detect lots of slow forming, but not many fast cancers • Because slow has better prognosis, it appears that screening helps outcome, but actually just selects a high proportion of slow cancers
Lead time • A screening test diagnoses something earlier but has no impact on outcome • Appears to increase survival time, but doesn’t Lead time Screened patients Non-screened patients Screening detects a disease Symptoms start Death
Overdiagnosis • Patients are diagnosed with a condition which isn’t going to affect their life expectance • e.g. prostate cancer diagnosis in old men • Get a PSA blood test done, high result but managing with symptoms ok • Now told they have cancer – anxiety, health insurance etc.
A new blood test is developed for rheumatoid arthritis. What is the sensitivity, specificity, PPV and NPV? Sensitivity = 250 / (250+3) = 98.8 % PPV = 250 / (250+26) = 90.5 % Specificity = 150 / (150+26) = 85.2 % NPV =150 / (150 + 3) = 98 %