Compatibility Testing
Compatibility Testing. Ahmad Shihada Silmi Msc, FIBMS IUG. What is compatibility testing?. Also called pretransfusion testing Purpose : To select blood components that will not cause harm to the recipient and will have acceptable survival when transfused

Compatibility Testing
E N D
Presentation Transcript
Compatibility Testing Ahmad Shihada Silmi Msc, FIBMS IUG
What is compatibility testing? • Also called pretransfusion testing • Purpose: • To select blood components that will not cause harm to the recipient and will have acceptable survival when transfused • If properly performed, compatibility tests will confirm ABO compatibility between the component and the recipient and will detect the most clinically significant unexpected antibodies
Compatibility testing? • There are several components of compatibility testing • Proper specimen collection • Reviewing patient transfusion history • ABO, Rh, and antibody testing (screen/ID) • Crossmatching • Actual transfusion
Compatibility testing • Can be divided into 3 categories: • Preanalytical procedures • Serological testing • Postanalytical procedures
Pre-analytical phases • Patient identification • Specimen collection • Review of patient history
Patient Identification • Must confirm recipient’s ID from bracelet ON the patient • Full patient name and hospital number • Name of physician http://www.usatoday.com/tech/news/techinnovations/2006-07-17-chips-everywhere_x.htm
Sample Identification • The sample should also have the full patient name, hospital number, and physician • Date and time of collection, phlebotomist’s initials • All of this should be on the request form and the sample
Specimen Tubes Pink Top - EDTA Red Top – no additives
Specimen Collection • Collected in tube with EDTA or no additives • If the venipuncture causes hemolysis, the sample may be rejected • True hemolysis in the patient is the result of complement activation • Samples are labeled at the bedside (pre-labeling is not recommended) • A record of individuals who collect (or test) the specimens should be documented in order to “backtrack” in case of an error
Specimen Collection • If the sample is drawn from an IV line, the IV infusion should be stopped 5-10 minutes prior to blood drawing and the first 10 mL discarded • Testing should be performed on samples less than 72 hours or else complement dependent antibodies may be missed (complement can become unstable)
Getting the history • Look at recipient’s records for any prior unexpected antibodies • Previous transfusion reactions
Serological Testing • 3 tests: • ABO/Rh • Antibody detection/identification • Crossmatch
ABO/Rh Typing • In the ABO typing, the forward and reverse MUST match • In the Rh typing, the control must be negative • Both of these will indicate what type of blood should be given
Antibody screen and/or ID • The antibody screen will detect the presence of any unexpected antibodies in patient serum • If antibodies are detected, identification should be performed using panel cells (with an autocontrol) • IS • 37° (LISS) • AHG • If an antibody is present, units negative for the antigen must be given • Proceed to the crossmatch…
Crossmatching • Purpose: • Prevent transfusion reactions • Increase in vivo survival of red cells • Double checks for ABO errors • Another method of detecting antibodies
Crossmatch • Two types of crossmatches • Major – routinely performed in labs • Minor – not required by AABB since 1976
Major vs Minor Crossmatch • Why is the minor crossmatch unnecessary? • Donated units are tested for antibodies • Most blood is transfused as packed cells, having little antibodies
Crossmatches • The AABB and FDA develop the standards for blood banking • According to the AABB Standards: The crossmatch “shall use methods that demonstrate ABO incompatibility and clinically significant antibodies to red cell antigens and shall include an antiglobulin phase”
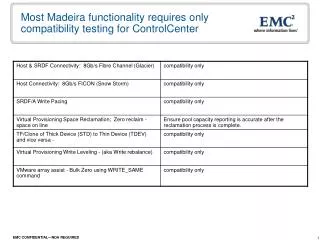
Crossmatch No agglutination ~ compatible Agglutination ~ incompatible Donor RBCs (washed) Patient serum
The procedure • Donor cells are taken from segments that are attached to the unit itself • Segments are a sampling of the blood and eliminate having to open the actual unit
Procedure • ABO/Rh typing is FIRST performed • Antibody Screen is performed next….
Crossmatch Procedure • if antibodies are NOT detected: • Only immediate spin (IS) is performed using patient serum and donor blood suspension • This fulfills the AABB standard for ABO incompatibility • This is an INCOMPLETE CROSSMATCH • If antibodies ARE detected: • Antigen negative units found and X-matched • All phases are tested: IS, 37°, AHG • This is a COMPLETE CROSSMATCH
Crossmatches… Will Verify donor cell ABO compatibility Detect most antibodies against donor cells Will Not Guarantee normal survival of RBCs Prevent patient from developing an antibody Detect all antibodies Prevent delayed transfusion reactions Detect ABO/Rh errors
Additional Information on Types of Compatibility Tests • Manual (IS and IAT) • Gel Technology • Electronic (Computerized) Cross match • Red cell Affinity Column Technology (ReACT) • Solid Phase Adherence Assays (SPAA)
Manual (IS and IAT) Antibody • IS detect RT reactive antibodies (Auto, Alloantibody, Naturally occuring) • IAT detect IgG antibodies (Auto & alloantibody) Acquired Naturally occuring (Cold agglutinin) Alloantibody Autoantibody
Gel Technology • Patient serum, and 1% of suspended RBCs in LIM are dispensed into the microtube and incubated at 37oC for 15 minutes. • The card containing the microtubes is then centrifuged at a controlled speed for 10 minutes. • At the start of centrifugation the cells are separated from the serum; then they meet the AHG contained in the microtube. • Finally the cells are trapped by the gel (if agglutinated) or pellet to the bottom of the tube.
X Match Phases clinically insignificant such as anti- M, -N, -Lea, -Leb, and -I. This phase is usually read only macroscopically for agglutination This phase is read microscopically for agglutination ` added to all negative tests and must produce a positive result
Limitations of Pretransfusion Testing • Hemolytic transfusion reaction, if the patient's antibody is too weak to be detected. • Standard antibody detection methods such as the indirect antiglobulin test require several 100 antibody molecules per red cell to produce detectable reactions. • A hemolytic transfusion reaction due to patient misidentification. For example, group A red cells (meant for transfusion to a group O recipient) will be compatible in vitro tests with an incorrect specimen drawn from a group A person.
Limitations of Pretransfusion Testing • Hemolytic transfusion reaction if donor red cells are inadvertently hemolysed before entering the patient, e.g., red cells hemolysed by an improperly functioning blood warmer or red cells hemolysed by contact with an ice pack in a transport container. • Nonhemolytic transfusion reactions such as allergic, febrile, and other reactions. • Pretransfusion test are meant to detect only red cell antibodies.
Incompatible cross match • ABO incompatibility • Recheck patient and blood unit ABO group • Clinically Significant Ab • DAT & IAT
IAT • IAT is used to detect clinically significant IgG antibodies bound to RBCS in vitro. • Detection of free Abs in patient's serum. • Clinically significant IgG Abs cause hemolysis or reduce survival of transfused RBCs, like D, c, E, K, k, JKa, JKb, FYa, FYb , S, s. • Unimportant Abs: I, P1, Lea, Leb, M, N. • Those Abs are Unimportant due to • Mostly cold reactive (IgM) • Could be neutralized
IAT is principally used for • Ab detection • Ab investigation (identification) • Ab titration • Compatibility testing • Phenotyping for some RBCs antigens
Reagent used in IAT Characteristics of RBCs reagent: • Three cell reagent sets, Serocyte I, II, III. • RBCs antigens corresponding to important and clinically significant Abs. • The reagent cells are suspended in saline and 2%-5% antibiotic. • Expired reagent should not be used. • An antigram defining phenotype of reagent cell must included with every cell. • All reagent should be stored at 1-6oC.
Performance IAT • Most clinically significant Abs react at 37oC, • RT and IS are not required. • AHG is usually monospecific IgG • No need for polyspecific AHG. Because • Anti C will detect Abs during the incubation phase. • Anti C enhance the detection of cold agglutinin such as anti I, anti P that are non significant Abs and not important in transfusion. • Delaying transfusion in critical situations.
Interpretation Result of IAT Negative IAT • OCC Positive: Report IAT negative Positive IAT Perform: • Ab identification. • Ab titration.
Interpretation Result of IAT • Low titer, and weak reactive Abs are failed to be detected • Using commercial reagents include RBCs that express important antigens in double dose, as JK (a + b -), JK Fy and Fy (a + b -), Fy (a + b -) cells. • Avoiding use of LISS LISS enhance reactivity of cold reactive Abs causing difficulties in detection clinically significant Abs . • Increase amount of serum to increase amount of Abs.
Its not a life threatening situation when an unexpected clinically important Abs to an RBCs Ags in a blood unit is not detected, Because • The plasma volume is small, and Abs will be diluted in recipient circulation • Unlikely to cause significant destruction to recipient's RBCs.
0.3% - 2.8% of the population are Ab makers, they produce clinically significant Ab. • Pregnancy and transfusion are the common cause of immunization to RBCs Ags.
Serological Properties Abs of blood groups vary in importance and significance due to serological properties • Temperature phase • 37oC reactive Abs as anti D, c, E, K, k, JKa, JKb, FYa, FYb , S, s. • Cold agglutinin as anti Lea, Leb, I, P1, M, N. • Inducing HDN and HTR • Activation complement. • Neutralizing by soluble blood group Ags
Problems Encountered • Autoantibody directed against own cell Ags solution • Elution IgG Abs can be dissociated from RBCs membrane Ags by physical or chemical means, some procedures destroy membrane, some leave it intact. Supernatant fluid (elute) contain the autoantibodies which can be identified..
Problems Encountered • Combination of auto and alloantibody solution • Treatment with ZZAP (Adsorption) ZZAP effectively removes autoantibodies (digestion) allowing more complete absorption of autoantibodies from patient's serum, allowing detection and identification of alloantibody. • Chemically treated allogenic RBCs Treated RBCS with proteolytic enzymes, alter some Ags
Problems Encountered • Weak or non reacted with any or some cell reagent. • Variable reaction • Variable expression of Ags (P1, Lewis) • Ags deteriorate on storage (Duffy, P1, M, Lewis) • Abs is reacting with more than one Ag. DDCCee 3+ Ddccee 1+ • Solution • Use double dose of corresponding Ags, (Rh, Kidd, • Duffy, MNS) • Use new cell reagent
Post-analytical phase • Involves labeling, inspecting, and issuing the blood unit • Labeling form includes patient’s full name, ID number, ABO/Rh of patient and unit, donor #, compatibility results, and tech ID • Form is attached to the donor unit and only released for the recipient • The unit is visually inspected for abnormalities, such as bacterial contamination, clots, etc