Download
1 / 20
210 likes | 488 Vues
Delivery Room Management of Neonates with Single Ventricle Physiology. John D. Loyd, MD, MPH Division of Neonatology Dell Children’s Hospital Seton Family of Hospitals. Prenatal Diagnosis. Fetal Echo 90-95% accurate When inaccurate initial management seldom changes

E N D
Delivery Room Management of Neonates with Single Ventricle Physiology John D. Loyd, MD, MPH Division of Neonatology Dell Children’s Hospital Seton Family of Hospitals
Prenatal Diagnosis • Fetal Echo • 90-95% accurate • When inaccurate initial management seldom changes • Forbus et al, AM J Cariol 2004; 94 • Perolo et al, Ultrasound Ob Gyn 2001; 18 • Rychik et al, J Perinatol 1997; 17
Prenatal Diagnosis • Similar: • Surgical mortality • Overall mortality • Duration of mechanical ventilation • Length of hospital stay • Decreased: • Lactate levels • Max BUN and Creatinine Eapen Am J Perinatol 1998;15, Mahle Pediatrics 2001;107, Kumar Am J Cardiol 1999;83, Verheijen Utrasound Ob Gyn 2002; 19.
Normal Fetal Circulation • Gas Exchange by placenta • Pulmonary vascular resistance high • Pulmonary blood flow low • Right ventricular output maintained by right-to-left shunt ductus arteriosus
Normal Transitional Circulation Fetal Life Newborn PA Pressure Blood Flow Oxygen Tension
Fetal Circulation with Single Ventricle Physiology • Generally well tolerated but the brain and mycardium see lower oxygen levels. • Have complete mixing versus the preferential shunting normally seen. • Severe AV regurgitation and mycoardial dysfunction are exceptions. • Possible somatic changes (poor head growth). • Rosenthal et al, Pediatrics, 1997; 100.
Ductus Arteriosus Lim et al, Arch Dis Child 1992; 67. Reller et al, J Pediatr 1993; 122. Gentile et al, J Pediatr 1981; 98.
Delivery Room Resuscitation • 5-10% of infants require some resuscitation. • Similar number with single ventricle physiology • Mirlesse reported on 110 infants with known CHD and only 11 required more than routine care. • Generally resuscitate according to NRP Am J Perinatol 2001; 18.
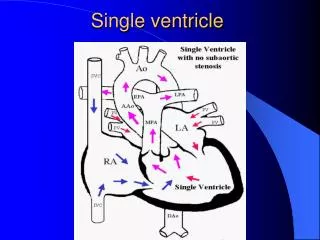
DDPBF Lower than normal saturations Start PGE1 DDSBF Lower than normal saturations Start PGE1 If atrial septum is restrictive then may need emergent BAS. Single Ventricle in the Delivery Room
Single Ventricle in the Delivery Room • Primary objective is to achieve good oxygen delivery. • Relative systemic and pulmonary pressures determine blood flow. • Typically saturations of 75-85% are seen with good pulmonary and systemic blood flow.
Oxygen • Remember that infants normally transition over a period of time. • Consider use of pulse oximetry. • Use oxygen very carefully as it may be detrimental to systemic blood flow.
Medications • Epinephrine and Bicarbonate are the only meds recommended by NRP. • Epi improves oxygen delivery in animal model of single ventricle physiology. • Bicarbonate may buy time but the underlying cause of the acidosis must be addressed.
Prostaglandin E1 • Has been approved for use in neonates to maintain the DA since 1981. • Must be administered via continuous infusion because 60-80% is metabolized during the first pass through the lungs.
More Common Side Effects Apnea-most common(~12%) Hypotension (capillary leak) Fever Rash Less Common Side Effects Gastric outlet Obstruction Cortical Hyperostosis Leukocytosis Seizures Prostaglandin E1
Prostaglandin E1 • Dose • Originally recommended 0.1mcg/kg/min • Many authors recommend starting at 0.01-0.015mcg/kg/min. • Acute side effects seem dose dependant. • Efficacy less dose dependant. • 500mcg of PGE1 in 82ml of D5W at the infant’s weight is 0.1mcg/kg/min. Hallidie-Smith, Arch Dis Child 1984; 59.
Location of Delivery • Recommended in a center where neonatal interventional cardiac services are available. Multiple citations to say this seems better. Mirlesse, Am J Perinatol 2001;18. • One report says it is reasonable to deliver most infants with CHD in non-surgical centers but this makes me nervous. Kelsall, Arch Dis Child 2000;82.
EXIT Procedure • Ex utero intrapartum treatment procedure • Used when immediate deterioration expected once placenta removed. • Children’s Hospital of Philadelphia.
Maternal Infant Bonding • Early interaction promotes bonding. • Better bonding likely improves the infant’s development. • Not studied in CHD as in healthy newborns. • Infant’s with CHD at risk for poor mother-infant interactions. • This may negatively impact development.
Bottom Line • Good communication important. • Most do well at delivery. • If infant doing well encourage parental interaction. • Obtain access. • Start PGE1 at 0.1-0.01mcg/kg/min • Observe for side effects and evidence of patent duct. • Obtain ECHO and adjust PGE1 if indicated.