Procalcitonin
Validation of a laboratory risk score for the identification of severe bacterial infection in children with fever without source. Galetto-Lacour A, Zamora S, Andreola B, Bressan S, Lacroix L, Da Dalt L and Gervaix A Arch Dis Child 2010; 95: 968-973 Dr Vanessa Craven. Procalcitonin.

Procalcitonin
E N D
Presentation Transcript
Validation of a laboratory risk score for the identification of severe bacterial infection in children with fever without source Galetto-Lacour A, Zamora S, Andreola B, Bressan S, Lacroix L, Da Dalt L and Gervaix AArch Dis Child 2010; 95: 968-973 Dr Vanessa Craven
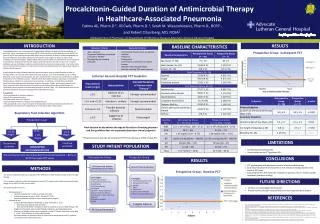
Pediatr Infect Dis J 2008; 27: 654-6 • 202 7- 36 months • Rectal temp >38°C & no focus • IOS • Urine MC&S • WCC, CRP & PCT • LP ‘when meningitis suspected’ • Clinical follow up within 48 hours
Results • SBI 54 (27%) • PCT: OR 37.6 (5.8 - 243) • CRP: OR 7.8 (2 - 30.4) • Urine dipstick: OR 23.2 (5.1 - 104.8)
AIM • External validation • More children • 2007 Italian population • Laboratory score ≥ 3
Methodology • Prospective enrolment - 408 children • Data from Italian study • May 2004 - October 2005 • 7 days (>38C) to 36 months (>39.5°C)
7 days to 36 months Fever without source Exclusion criteria Looking for severe bacterial infection (defined) – diagnosis ‘at end of follow up’ SBI vs ‘benign viral infection’ Retrospective (5 years) Using another study’s cohort
Reasonable age definition & exclusion criteria Using another study’s data set Higher temperature cut off than used in practice?
Laboratory measurements Who confirmed FWS? ALL were assessed at 72 hours (including telephone contact) – no details Cultures would be back but not always reliable What happened to the classification of children that did not improve? Or had focal infection and did not get Abx DMSA to diagnose pyleonephritis (1/52)
Who did the assessments? Who followed up?
ALL were followed up No details about - follow up length - location Was 72 hr review conclusive in all Any need Abx/admission What happened to the ‘focal bacterial infection’ 15.8%?
SBI in 92 (22.7%) Score ≥3: Sens 86% (77-92%) Spec: 83% (79-87%) Sens ↑and spec ↓ with age WBC: Sens 52%, Spec 75% CRP: Sens 52%, Spec 75% PCT: Sens 75%, Spec 76% Missed 13 cases Very large confidence intervals! Large confidence intervals Selected population
BUT referral pathway different WCC poor predictor Pediatr Infect Dis J 2008; 27: 654-6 Results comparable to derivation set
Summary & Conclusion There is insufficient evidence to support the sole use of the lab score to identify those with severe bacterial infection