Download
1 / 56
591 likes | 1.13k Vues
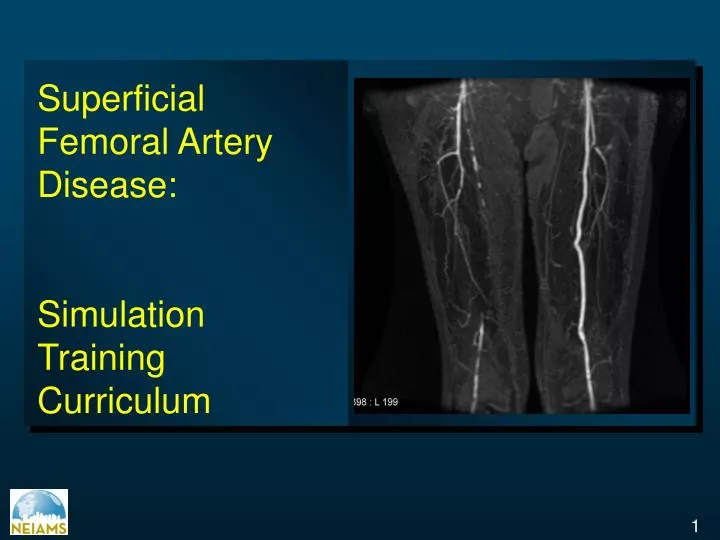
Superficial Femoral Artery Disease: Simulation Training Curriculum. Superficial Femoral Arterial Disease. Prevalence Clinical Presentation Diagnosis Indications Technical Issues Treatment Options - PTA - Surgical Complications Prognosis.

E N D
Superficial Femoral Artery Disease: Simulation Training Curriculum
Superficial Femoral Arterial Disease Prevalence Clinical Presentation Diagnosis Indications Technical Issues Treatment Options - PTA - Surgical Complications Prognosis
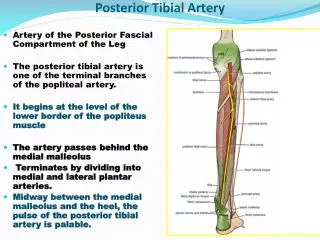
SFA disease: Responsible for > 50% of PAD Cases • One of the longest vessels in the body • Torsion/compression/flexion/extension by the largest muscle group • Two flexion points • Few collateral sources • Occlusions predominate
Superficial Femoral Arterial Disease • Most common in men than women • Most common in older patients with concomitant coronary disease • Strong relationship between increased tortuosity and disturbed hemodynamic patterns in regions of the SFA Predilection for the region of the adductor canal 1 1. Wood et al J Appl Physiol 2006 (6)
3. Extension / Contraction 1. 2. Flexion Torsion 4. Compression Forces Exerted in SFA
Superficial Femoral Arterial Disease • Isolated SFA disease predicts low amputation risk (0-1%) without surgical revascularization 1 • Cumulative smoking history • Contralateral superficial femoral artery occlusion • Presence of diabetes • DISEASE PROGRESSION • Other arterial segments involved • Increasing risk of critical limb ischemia 1. Hertzer NR Circulation 1991; 83(Suppl.1):I-12 – I-19
Superficial Femoral Arterial Disease Prevalence Clinical presentation Diagnosis Indications Technical Issues Treatment Options - PTA - Surgical Complications Prognosis
Clinical Presentation • Claudication • Critical limb ischemia (less common) • The presence of the Profunda Femoris Artery, the main nutritive artery of the thigh, protects patients with SFA occlusion from critical limb ischemia
Morphological Stratification of Femoropopliteal Lesions ACC/AHA Guidelines
Superficial Femoral Arterial Disease Prevalence Diagnosis Indications Technical Issues Treatment Options - PTA - Surgical Complications Prognosis
Superficial Femoral Arterial Disease:Diagnosis • Clinical evaluation Stevens et al JAMA 2006;295(5):584
Diagnostic Methods • Ankle-and Toes – Brachial Indices, segmental pressure examination • Pulse volume recording • Continuous wave doppler ultrasound • Treadmill exercise testing with and without ABI assessments and 6 minute walk test • Duplex ultrasound • Computed tomographic angiography • Magnetic resonance angiography • Contrast angiography Hirsh et al Circulation 2006; 113(11): e463-654 ACC/AHA Guidelines
Diagnostic Methods: Duplex Ultrasound Stenosis in the superficial femoral artery visualized satisfactorily in the color mode Ramaswami et al J Endovasc Surg. 1995; 2(1): 27-35
Diagnostic Methods: MRA Lower extremity MRA showing severe stenoses in left superficial femoral artery and smaller stenoses in right superficial femoral artery. Cochrane J Radiology Rounds MGH 2004;2(11)
Diagnostic Methods: CTA • The diagnostic accuracy of CT angiography has been proved superior to that of conventional arteriography in several applications • CT angiography is substantially less invasive and less expensive, and it allows three-dimensional visualization from any angle and in any direction, which cannot be achieved with projection techniques such as DSA Coronal multi–detector row CT angiography : Occlusion of the right superficial femoral artery (thick arrow) Catalano et al Radiology 2004;231:555-563
Diagnostic Methods: DSA A B Digital subtraction angiography (DSA) shows A the occlusion of the left common iliac artery and external iliac artery, long occlusion of both superficial femoral arteries (SFAs) with no visible stump on the left, and B restoration of both distal SFAs through collaterals (arrows) Yılmaz et al Eur Radiol. 2002;12(4): 911-4
Superficial Femoral Arterial Disease Prevalence Diagnosis Technical Issues Treatment Options - Medical - PTA - Surgical Complications Prognosis
Superficial Femoral Artery Technical Approach • Diagnostic Arteriogram: Showing inflow and outflow of the target lesion • Run-off angiography to visualize the lower extremity circulation Grossmans “Catheterization” 7th Ed. pg. 254-280
Vascular Access • Antegrade common femoral artery puncture : • Most common • Contralateral retrograde access over the aortic bifurcation • Advantages: • The ability to image the common femoral and its bifurcation • The ability to treat iliac and infrainguinal disease in the same timing • Disadvantages: • Working from a distance with exchange-length wires and balloons • Retrograde popliteal artery access • Rare cases where the antegrade or contralateral approach fails to traverse an occluded segment • In the event that a subintimal channel has been created • Brachial access • Provides better radiation protection, since one is working far from the actual target site, but requires the use of lengthy wires and devices
Superficial Femoral ArteryAnticoagulation • Aspirin (325 mg) once a day several days prior the procedure • After access has been obtained and prior to intervention: 2500 – 5000 international units of heparin
Superficial Femoral Arterial Disease Prevalence Diagnosis Technical Issues Treatment Options - Medical - PTA - Surgical Complications Prognosis
Superficial Femoral Arterial Disease: Treatment Patients with Claudication • Aggressive risk factor modification • Exercise program Patients with Critical Limb Ischemia • Revascularization
Superficial Femoral Arterial Disease:Angioplasty • PTA is the preferred initial treatment in patients with disabling claudication 1 • In patients with critical leg ischemia, PTA is better for the treatment of femoropopliteal stenosis, whereas femoropopliteal occlusion is best managed with bypass grafting 1 • Percutaneous transluminal angioplasty (PTA) has been recommended only for short lesions of the superficial femoral artery 2 1. Hunink et al JAMA 1995; 274(2) 165-171 2. Dormandy JA, Rutherford B J Vasc Surgery 2000; 31:S1-S296
Superficial Femoral Arterial Disease:Angioplasty • Low procedural morbidity and mortality • Reduced costs • Shortened hospital stay • Preserves collaterals so that even if the angioplasty site occludes, symptoms might not return • Patients who are expected to live for less than 1–2 years and have significant comorbidity should probably, when possible, be offered angioplasty first. If the procedure fails, the patient may not be disadvantaged in the short term and can go on to have surgery if regarded as appropriate Adam et al Lancet 2005;366:1925-1934.
Adjunct Therapies • Stents • Directional atherectomy • Rotational atherectomy • Laser angioplasty • Intra-arterial radiation • Cryotherapy
Superficial Femoral Arterial Disease:Stenting • Is recommended only as a bailout procedure after technical failure of angioplasty • Flow limiting dissections • Residual pressure gradient >15mmHg • Remaining stenosis >30% • An elastic recoil as well as failure to maintain initial patency Heuser R, Biamino G. Peripheral Vasc Stenting.2nd Ed. 91-108
The Palmaz TM stent High radial force: valuable in highly calcified lesions Precise placement Disadvantage: significant stiffness Strecker TM stents Very flexible: Allows for a contralateral placement using crossover approach Disadvantage: deformability by extrinsic compression, which can lead to restenosis and reocclusion in the femoropopliteal tract Superficial Femoral Arterial Disease: Balloon Expandable Stents : Not indicated in the femoropopliteal region, with exception of short, very calcified lesions less than 2 cm in length. Heuser R, Biamino G. Peripheral Vasc Stenting.2nd Ed. 91-108
Superficial Femoral Arterial Disease:Stenting • Stents of choice for implantation in the SFA • Advantages over balloon expandable stents: • Higher flexibility • Recoil tendency after external deformation The Wallstent • Difficult exact placement: shortening up to one-third Ninitol Stents • Implantation more precise foreshortening (Max 5%) • Superior accommodation to different artery diameters
Duplex-guided Balloon Angioplasty and Stenting • Duplex methodology can be used to map the arterial disease process and to guide wires, sheaths, balloons, and stents for the treatment of superficial femoral • Effective in achieving excellent anatomic and hemodynamic improvement regardless of the extent of the stenotic lesion • Benefic in patients severely allergic to contrast material or those with renal insufficiency Power Doppler image of severe (81%) superficial femoral artery stenosis. The hemodynamic significance of this lesion was confirmed by a peak systolic velocity of 388 cm/s with marked spectral broadening. Ascher et al J Vasc Surgery 2005; 42(6): 1108-1113
Directional Atherectomy Directional atherectomy of right superficial femoral artery. A. Angiography via antegrade punctureinto right common femoral artery demonstartes high-grade stenosis in proximal SFA, not favorable for balloon angioplasty owing to ostial location/eccentricity. B. An 8Fr directional atherectomy catheter introduced via sheat, which is then pulled back to common femoral artery. C. Angiography following DA demonstrates excellent result Grossmans “Catheterization” 7th Ed. pg. 593-595.
Excimer laser Atherectomy Excimer laser atherectomy of peripheral arteries has been practiced commercially in Europe since 1994 and has been shown to be a useful adjunct for the treatment of long superficial femoral artery (SFA) occlusions Scheinert et al JEndovasc Ther. 2001;8:156–166
Superficial Femoral Arterial Disease: • When PTA has been attempted for more diffuse disease and long occlusions, limb salvage rates are considerably lower Laird et al J Endovasc Ther. 2006 Feb;13(1):1-11
A) A rather extreme case of severe ulceration with associated infection on the bottom of the foot prior to intervention. (B) At 6 months after treatment with excimer laser atherectomy , healing is nearly complete Laird et al J Endovasc Ther. 2006 Feb;13(1):1-11
Surgery • Bypass surgery with venous grafts • Good long-term anatomical patency • Clinical durability • Bypass surgery vs. angioplasty : • Angioplasty also seems to be a much less expensive option than surgery, at least in the short term • The rates of amputation – free survival after surgery and balloon angioplasty are similar for the first two years. Adam et al Lancet 2005;366:1925-1934.
Amputation-free survival after bypass surgery and balloon angioplasty Adam et al Lancet 2005;366:1925-1934.
All-cause mortality after bypass surgery and balloon angioplasty Adam et al Lancet 2005;366:1925-1934.
Poor Surgical Candidates • Severe distal tibial occlusive disease • Inadequate distal targets for revascularization, • Absent venous conduit, or • Significant medical or cardiac comorbidities rendering them at high risk for complications from surgery. Laird et al J Endovasc Ther. 2006 Feb;13(1):1-11
Superficial Femoral Arterial Disease Prevalence Diagnosis Technical Issues Treatment Options - Medical - PTA - Surgical Complications Prognosis
Complications • Acute or subacute thrombosis • Restenosis • Dissection • Distal embolization • Perforation • Hematoma • Stent fractures
Superficial Femoral Arterial Disease Prevalence Diagnosis Technical Issues Treatment Options - Medical - PTA - Surgical Complications Prognosis
Unfavorable Predictors • Type of lesion (occlusion) • Long or eccentric lesions • Diffuse atherosclerosis • Limb-threatening ischemia • Poor initial post-PTA appearance • Diabetes mellitus • Congestive heart failure • Poor distal outflow
Favorable Predictors • Higher preoperative ABI • Performance of angioplasty • Type of lesion (stenosis)
Percutaneous angioplasty or stenting of the SFA 1986-2004 Primary Patency Rates (%) Months 380 limbs 66% IC Surowiec SM. J Vasc Surg. 2005;41(2):269-78
SFA Patency Rates Meta-analysis 1993-2000 3-year Primary Patency Rates Roehring JVS 2005
Rates of Restenosis on Angiography Angiplasty Stenting P=0.05 P=0.02 Restenosis Rate % 43% (23 of 53) 24% (12 of 51) 50% (18 of 36) 25% (17 of 68) Schillinger et al N Eng J Med 2006;354:1879-1888
Rates of Restenosis on Duplex Ultrasonography Angioplasty Stenting P=0.36 P=0.06 P=0.01 Restenosis Rate % 23% (12 of 53) 14% (7 of 51) 45% (24 of 53) 25% (13 of 51) 63% (33 of 52) 37% (18 of 49) Schillinger et al N Eng J Med 2006;354:1879-1888
P=0.25 P=0.68 P=0.50 P=0.04 P=0.04 Clinical Outcomes Angioplasty Vs Ninitol Stent Group Maximum Walking Distance (m) Schillinger et al N Eng J Med 2006;354:1879-1888
SFA PTA or Stenting 1986-2004 Comparison with Venous and Prosthetic Bypass TASC LESION TASC LESION Surowiec SM. J Vasc Surg. 2005;41(2):269-78
Stent or PTA of the SFA 1986-2004: Freedom from symptom recurrence TASC lesion Surowiec SM. J Vasc Surg. 2005;41(2):269-78
Durability of Endovascular Intervention for Iliac and Femoropopliteal Disease Primary Patency at 1, 3, 5, Years TASC Working Group , J Vasc Surg 2000;31:S1-S296