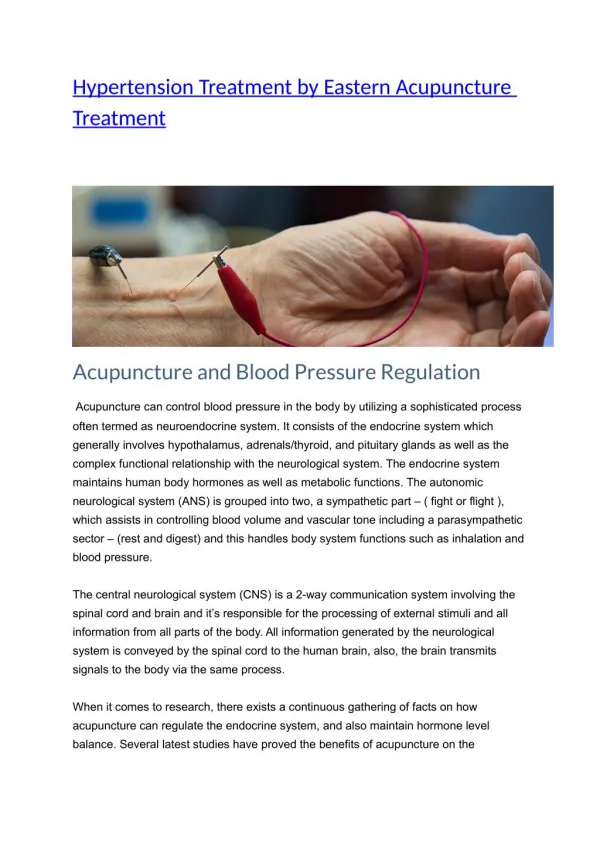
Hypertension Treatment
340 likes | 751 Vues
Hypertension Treatment. Dr.Negin Nezarat. mechanisms and cardiovascular pathophysiology (Review ). major forms of clinical hypertension. major classes of anti-hypertensive agents and mechanisms of action 4. General treatment strategy for hypertension. Determinants of Arterial Pressure.

Hypertension Treatment
E N D
Presentation Transcript
HypertensionTreatment Dr.NeginNezarat
mechanisms and cardiovascular pathophysiology (Review). • major forms of clinical hypertension. • major classes of anti-hypertensive agents and mechanisms of action • 4. General treatment strategy for hypertension.
Determinants of Arterial Pressure Blood Volume Mean Arterial Pressure = X Arteriolar Diameter Stroke Volume Heart Rate CRITICAL POINT! Change any physical factors controlling CO and/or TPR and MAP can be altered. Contractility Filling Pressure Blood Volume VenousTone
1. Neural SymNS PSNS 2.Hormonal Renal Ang II Adrenal Catecholamines Aldosterone 3. Local Factors Artery Vein Mechanisms Controlling CO and TPR
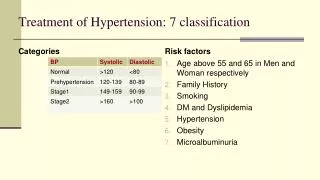
Types and Etiology of Hypertension White coat hypertension Secondary hypertension 1. renal artery stenosis 2. pheochromocytoma 3. aortic coarctation 4. adrenal tumor Essential Hypertension No known cause. CRITICAL POINT! Pharmacological Therapy used primarily for essential hypertension.
1. Diuretics 2.Peripheral a-1 Adrenergic Antagonists 3. Central Sympatholytics (a-2 agonists) 4. b-Adrenergic Antagonists 5. Anti-angiotensin II Drugs 7. Vasodilators 6. Ca++ Channel Blockers
Diuretics Urinary Na+ excretion Urinary water excretion Extracellular Fluid and/or Plasma Volume Acute decrease in CO Chronic decrease in TPR, normal CO Mechanism(s) unknown
1. Thiazides hydrochlorothiazide chlorthalidone metolazon 2. Loop diuretics furosemide(Lasix) bumetadine ethacrynicacid 3. K+ Sparing amiloride , spironolactone (Aldactone); triamterene 4. Osmotic mannitol ,urea 5. Other Combination - HCTH + triamterene acetazolamide (Diamox)
dizziness, electrolyte imbalance/depletion, hypokalemia, hyperlipidemia, hyperglycemia (Thiazides) gout
Contraindications hypersensitivity compromised kidney function cardiac glycosides (K+ effects) hypovolemia hyponatremia
A 55 y/o Hypertensive man under HCT TX • BP:160/95 • Peripheral Edema • Cr:1.3 • Na:129 • K:3.2 • lower dietary Na+ intake, • K+ supplement or high K+ food • K+ Sparing • Loop diuretics (severe HTN,CRF or with CHF)
Peripheral a-1 Adrenergic Antagonists Prazosin Terazosin Vasodilation reduces peripheral resistance
Peripheral a-1 Adrenergic Antagonists nausea; drowsiness; postural hypotenstion; 1st dose syncope Orthostasis Volume overload CHF does not impair exercise tolerance useful with diabetes, asthma, and/or hypercholesterolemia often used with diuretic, antagonist
Central Sympatholytics (a-2 Agonists) Clonidine , Methyldopa ,Guanfacine Sympathoinhibition Decreased norepinephrine release Decreased NE-->vasodilation--> Decreased TPR
Dry mouth Sedation Impotence Generally Not 1st Line Drugs; Methyldopa Drug Of Choice For Pregnancy prolonged use--salt/water retention, add diuretic Rebound increase in blood pressure
b Adrenergic Antagonists propranolol (Inderal) Pindolol Metoprolol Atenolol Carvedilol labetalol
Impotence; Bradycardia; Fatigue; Exercise Intolerance, Hypertriglyceridemia, Cardiac-- HR, SV CO Renal-- Renin Angiotensin II TPR
Asthma Bradycardia Hypersensitivity Hypoglycemia in DM
2. Ang II Receptor Antagonists losartan candesartan valsartan (Diovan) Anti-Angiotensin II Drugs Angiotensin II Formation Angiotensin Converting Enzyme- Inhibitors enalopril quinapril fosinopril moexipril lisinopril benazepril captopril Ang I Angiotensinogen ACE Lung VSM Brain Kidney Adr Gland Ang I AT1 Ang II ACE AT2 Ang II Renin
Anti-Angiotensin II Drugs, cont Angiotensin II Volume Aldosterone Vasopressin HR/SV Angiotensin II Norepinephrine Vasoconstriction SymNS SymNS CO TPR CO
Adverse Effects hyperkalemia angiogenic edema (ACE inhib); cough (ACE inhib); rash; itching; Pregnancy,hypersensitivity,bilateral renal stenosis Use With Diabetes Or Renal Insufficiency; Adjunctive Therapy In Heart Failure; Often Used With Diuretic; Enalapril, Iv For Hypertensive Emergency
A 25 y/o hypertensive woman under low dose diuretic and 12.5 mg captopril • Positive pregnancy test • BP:125 / 75 • Contraindications in pregnancy for ACEI & ARB • Continuse diuretics • Add methyldopa if necessary
Ca++ Channel Blockers Verapamil Nifedipine Diltiazem Amlodipine K+ Ca++ Na+ Vascular Relaxation Decreased TPR
Adverse Effects nifedipine --Increase SymNS activity; headache; dizziness; peripheral edema Contraindications Congestive heart failure; pregnancy and lactation; Post-myocardial infarction Therapeutic Considerations Verapamil- Mainly Cardiac; Interactions W/ Cardiac Glycosides Nifedipine- Mainly Arterioles,reflex Tachycardia Diltiazem-both Cardiac And Arterioles,AV Node Block
NO Vasodilators Hydralazine ,Minoxidil ,Nitroprusside ,Diazoxide , Fenoldopam nitroprusside fenoldopam DA minoxidil diazoxide K+ Na+ Ca++ Ca++ hydralazine
Adverse Effects reflex tachycardia Increase Symactivity (hydralazine, minoxidil,diazoxide) lupus (hydralazine) hypertrichosis (minoxidil) cyanide toxicity (nitroprusside)
Summary Sites and Mechanisms of Action Can alter CO/TPR at number of sites and/or mechanisms. 3. -2 agonists Receptor antag. 2. a-antag. 5. ang II antag. 7. Vasodilators 6. Ca++ antag. 4. b-blockers 1. Diuretics 4. b-blockers Other- 5. ACE inhibitors Lung, VSM, Kidney, CNS CRITICAL POINTS!
When we have to start drug administraton for HTN? • Don’t response to goal with life style modification • > 160/100 at first