Download
1 / 54
590 likes | 858 Vues
Learn about oxidative stress, antioxidants, inflammation, and diabetes. Discover the clinical importance of CRP and antioxidants in managing diabetes complications. Explore the impact of lifestyle factors on inflammation and diabetes.

E N D
Inflammation an oxidative stress in diabetes? Naveed Sattar Professor of Metabolic Medicine Hon. Consultant in Clinical Biochemistry ABCD meeting October 2005
Outline • Oxidative stress (free radicals) • Any clinical value of antioxidants • Inflammation and diabetes • Any clinical use of CRP • Light overview
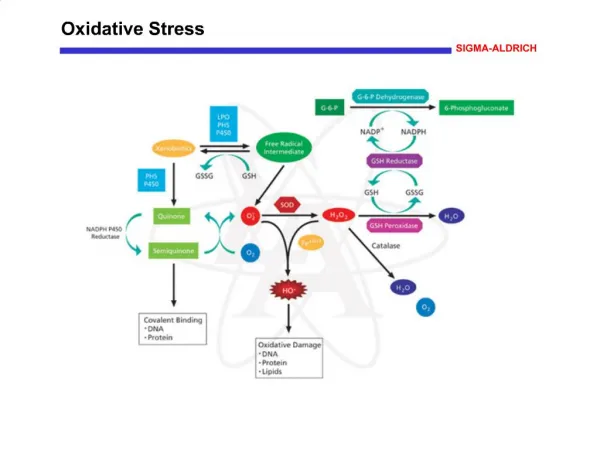
Why does oxygen damage? • O2 metabolism: • - Creates free radicals • - Not prejudicial • Interact with nearest molecule Not all free radical are bad! NO.
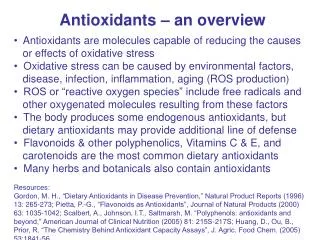
Antioxidants • endogenous enzymesexogenous • SOD vitamin C • Catalase tocopherols • circulating molecules carotenoids • albumin flavanoids • urate • bilirubin
Oxidative stress Protein lipid DNA carbohydrate Oxidised LDL mutations CHD Cancer Aging process
Homeostasis Oxidative stress Antioxidants Aging chronic diseases - CHD - Diabetes Maintain health
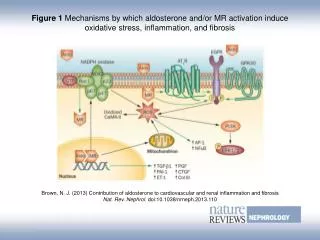
Oxidative stress linked to all diabetes complications Stroke DiabeticRetinopathy NFkB apoptosis Cataracts Lens Polyol CardiovascularDisease Oxidsed, glycated LDL AGEs Diabetic Nephropathy DiabeticNeuropathy H2O2 PKC pathways Mesangial cells ANGII> NADP(H) Glial cells Seen with Glial fibrillary acid protein Beta cell dysfunction via mitochondrial ROS Rahmi et al Biomed and Pharmacotherapy 2005
Hyperglycaemia with uraemia: double trouble Krane & Wanner (2002) NDT
Oxidative stress Antioxidants Aging chronic diseases - CHD - Diabetes Maintain health
Theory! Vitamin supplements + endogenous antioxidants Oxidative stress chronic diseases better health
Uncontrolled prospective studies US Nurses health study follow-up >100 IU/d vitamin E for ≥2 years significantly lowered risk of coronary events in males and females
Primary prevention Project - Italian [Lancet Jan 2001] 4495 age 64.4 with with CHD risk factors Aspirin 3.6 years Vitamin E 300 mg/d
b carotene Vitamin E CHD end-points
Stroke All cause mortality Other end-points
Thioctic acid (a-lipoic) and diabetic neuropathy • Water and lipid soluble • Disulphide bond • Works at level of mitochondria • Esp. well at peripheral nerves • 7 trials: recent meta-analysis n=1258 in RCTs • Significant benefit • Methods sub-optimal • Large USA trial on the go – “NATHAN” Ziegler Treat Endocrinol 2004
Where now for oxidation hypothesis? • “give earlier” • “higher doses” • “give for longer” • “wrong choice of antioxidants” • MAY work in some diseases • - pre-eclampsia (large trials ongoing) • - haemodialysis • HIV • Diabetic neuropathy?
Bypass GI & renal tracts
Oxidative hypothesis – summary so far • oxidative stress in diabetes – downstream of other pathways • Supplementation with antioxidants of unproven benefit • Stick with glycaemic control, lifestyle improvements & proven therapies
Outline • Oxidative stress • Any clinical value of antioxidants • Inflammation and diabetes • Any clinical use of CRP
Inflammatory marker in clinical useCRP as marker of inflammatory activity CRP ~20 mg/l minor surgery or infection CRP ~100 mg/l major surgery or sepsis CRP <6 mg/l “normal range”
hs-CRP and Risk of Future Cardiovascular Events in Apparently Healthy Women P Trend <0.002 6 Any Event 5 MI or Stroke 4 Relative Risk 3 2 1 0 1 2 3 4 <1.55 1.55–3.7 3.8–7.3 >7.3 Quartile of hs-CRP (Range, mg/L) Ridker. Circulation. 1998;98:731–733.
Cellular and molecular make-up of unstable plaques CRP, IL-6, IL-15, IL-18, MMPs etc
Lipoprotein(a) Homocysteine Total Cholesterol Fibrinogen tPA Antigen TC/HDL-C hs-CRP hs-CRP + TC/HDL-C 1.0 2.0 4.0 6.0 0 Relative Risks of Future MI among Apparently Healthy Middle-Aged Men: Physicians' Heart Study Relative Risk for Future MI Adapted from Ridker PM. Ann Intern Med 1999;130:933-937.
"Regression to the truth" John Danesh et al. C-Reactive Protein and Other Circulating Markers of Inflammation in the Prediction of Coronary Heart Disease NEJM 2004
Adipocytes circa 1990 Confounding factors FFA FFA Triglyceride
1. Obesity vs CRP levels 20-30% 25 20 15 Percent with CRP 2.2 mg/L 10 5 0 Normal Overweight Obese Visser M et al. NHANES 1988-1994JAMA 1999;282:2131-2135.
Inflammatory markers • Lifestyle factors • Obesity • Sedentary behav. • Poor diet • Low social class • Race CHD Alternative Mechanisms Lipids, BP, etc
Inflammation and diabetes • Do inflammation markers predict diabetes? • Any evidence that lessening inflammation improves insulin sensitivity?
Age Obesity Low physical activity FH diabetes South Asians Others PCOS High GI diet Diabetes CRP goes up with:
South Asians and CRP CRP mg/l P=0.05 3.5 3 2.5 2 1.35 mg/l 1.5 0.70 mg/l 1 0.5 0 Asians European Forouhi NG, Sattar N, McKeigue P. Int J Obesity 2001;25:327-31.
Does CRP predict new diabetes 139 subsequent All 5,974 diabetes subjects Age (years) 55.6 (5.7) 55.2 (5.5) Glucose (mmol/l) 5.49 (0.69) 4.72 (0.51) Body Mass Index (kg/m2) 27.7 (3.6) 25.9 (3.1) Ln sensitive CRP [ln(mg/l)] 1.05 (0.90) 0.53 (1.08)
Diabetes risk by CRP quintiles (mg/l) 1.00 < 0.66 1.76 0.66-1.3 2.35 1.3 -2.3 2.75 2.3 - 4.2 3.07 > 4.2 2.0 3.0 0.5 1 Adjusted Hazard Ratio
Kaplan-Meier curve % diabetic > 4.2mg/l 5 4 2.3 - 4.2 3 1.3 -2.3 2 0.66-1.3 1 < 0.66mg/l 0 0 0.5 1 1.5 2 2.5 3 3.5 4 4.5 5 Years in study Freeman DJ, Norrie J, Gaw A, Ford I, O'Reilly DS, Packard CJ, Sattar N; Diabetes. 2002
Multivariate Predictors of Diabetesin WOSCOPS 1.00 TC P = 0.95 0.86 HDL-C P = 0.24 1.55 Ln TG P = 0.0048 1.29 BMI P = 0.0006 1.14 Ln WBC P = 0.19 1.30 Ln CRP P = 0.001 1.5 2 0.5 1 Hazard Ratio Freeman DJ, Norrie J, Gaw A, Ford I, O'Reilly DS, Packard CJ, Sattar N. Diabetes 2002
Plausible Mechanisms? NEFAs Insulin Glucose uptake IL-6 Adipose stores + IL-6sR TNF-a TNF-a sR-I leptin Skeletal muscle IL-10 TNF-a “Functional pleiotropy” monocytes
LOCAL FAT TO INFLAMMATON TO INSULIN RESISTANCE Yudkin et al (2005) Lancet
Insulin resistance may lead to inflammation monocytes Pancreas Insulin Adiposetissue Glucose uptake FFAs Muscle Liver TG
e.g. Lipids type 2 diabetes Risk factor (obesity, etc) Inflammatory markers Inflammatory markers Inflammatory markers Risk factor (e.g. obesity, Low physical activity) Insulin resistance Diabetes