Download
1 / 37
370 likes | 488 Vues
Next Steps for Adolescent and Young Adult Oncology Basic Biology September 16-17, 2013. BBWG Members. Cary Anders Charles Mullighan Donald Blair Nita Seibel Archie Bleyer Beverly Teicher Lisa Boardman Magdalena Thurin Brandon Hayes- Lattin James Tricoli

E N D
Next Steps for Adolescent and Young Adult OncologyBasic BiologySeptember 16-17, 2013
BBWG Members Cary Anders Charles Mullighan Donald Blair Nita Seibel Archie Bleyer Beverly Teicher Lisa Boardman Magdalena Thurin Brandon Hayes-Lattin James Tricoli Javed Khan Cheryl Willman SivaaniKummar Stephen Hunger Melinda Merchant
AYA Survival Disparities • Acute Lymphocytic Leukemia • Children have an 80% cure rate • Teenagers and young adults have a five year survival rate of only 50% • Ewing’s Sarcoma • Five year survival rate • <10 years old 70% • 10-17 years old 60% • >18 years old 44%
Explanation for this Phenomenon • Low enrollment for this age group in clinical trials • 30-50% of child cancer patients participate • 1-2% of AYA cancer patients participate • Distinctive biology for these patients and their tumors • Developmental and hormonal differences
History • NCI Progress Review Group report on AYA Cancers, 2006 (NCI and Lance Armstrong Foundation) • NCI Adolescent and Young Adult Oncology (AYAO) working group formed in 2006 • NCI/Lance Armstrong Foundation AYA Cancers Workshop, June 9 and 10, 2009 • Publication of the AYA Workshop paper “Unique Characteristics of Adolescent and Young Adult Acute Lymphoblastic Leukemia, Breast Cancer, and Colon Cancer” JNCI 103: 628-635, 2011
What is known about the incidence, outcome and molecular characterization according to patient age of CRC in the AYAO age group? • Comprise 2-6% of total annual colorectal cancer (CRC) cases • Approximately 800 deaths annually • Poorer prognosis and more aggressive disease than in adults • Greater frequency of the following than in adult CRC • Mucinous and signet ring histology • Microsatellite instability high (MSI-H) • Mutations in Mis-match repair (MMR) genes • Lower frequency of the following than in adult CRC • K-ras mutations, 17p and 18q LOH • Lower p53 protein levels than found in adult CRC
Are there current studies investigating the molecular characterization of this tumor type in the AYAO age group? • Hill et al., Journal Clinical Oncology, 2007 • 77 CRC patients age 7-20 (St. Jude Children’s) • 48/77 (62%) displayed mucinous histology • 34/48 (71%) displayed signet ring histology (11-13% in adult CRC) • Did significantly more poorly than adult CRC patients despite being on adult protocols • Liu et al., Nature Medicine,1995 • 189 CRC patients with no evidence of HNPCC analyzed using 4-5 microsatellite markers per tumor (Johns Hopkins) • 31 patients were 35 or younger • 18 (58%) displayed MSI • 46 patients were 36-55 • 8 (17%) displayed MSI • 112 patients were 55 or older • 11 (10%) displayed MSI
What are the current studies ongoing in older or younger age groups that would provide further insight into the biology of this tumor? • The Cancer Genome Anatomy (TCGA) project has provided data on genes that are frequently mutated in adult CRC • TCGA has identified several genes that exhibit amplification and elevated expression in adult CRC, including IGF-2 • There are also consensus gene sets that exhibit mutations in adult CRC that have been identified (Vogelstein)
Clinical Questions • What contributes to the more aggressive clinical nature of AYA CRC tumors? • How can we better predict disease response in this group of patients? • What are the underlying reasons for the poor therapeutic response in this group of patients?
Scientific Questions • Why such a high frequency of MSI in the AYA group? • Hypermethylation of hMLH1 gene known to occur • What about other MMR genes? • What are the molecular reasons for poorer outcome for MSI-H patients in the AYA group? • What is the reason for the high frequency of the mucinous phenotype in the AYA group? • Why the difference in p53, K-ras and DCC characteristics in the AYA group?
What is known about the incidence, outcome and molecular characterization according to patient age of Breast Cancer in the AYAO age group? • Breast cancer is the most frequent cancer in women in the AYA population • ~1 in 200 AYA women will develop breast cancer • The disease is more likely to be aggressive, and to exhibit a triple negative, basel-cell phenotype • It often presents at a higher grade with a poorer prognosis • Molecular studies suggesting a novel gene expression pattern in AYA breast cancers have been controversial
Are there current studies investigating the molecular characterization of this tumor type in the AYAO age group? • Differential gene expression studies have investigated whether there is a unique pattern for AYA breast tumors in comparison to older women, but the results are conflicting and controversial [Anders et al, J. Clin. Oncol 2011,29:e18-e20; Azim Jr. et al, 2012 Clin Ca Res, 2012 1341-1351; Servant et. al. 2012 Clin Ca Res 1704-1715; Colleoni and Anders, the Oncologist 2013, 18:e13-15] • Studies suggest an association between germline TP53 mutations and early onset HER2-positive breast cancer, which could lead to elucidation of molecular pathways involved in breast cancer [Cancer 2012, 118(4): 908–913; Rath et al Breast Ca Res Treat 2013 139(1):193-198] • BRCA mutations have been linked to susceptibility and early onset of breast cancer [Infante et al. Breast Ca Res 2010 122(2):567-571, Andres et al Clin Transl Onc, 2013,10.1007/s12094-013-1070-9, ]
Clinical Questions • Do women in the AYA population show different responses to therapy than older patients despite the fact that the biology of the tumor itself appears to be similar? • Can the response of AYA patients to current therapies inform us about underlying mechanisms in this population • Can we identify a biological basis for the apparent greater tendency for AYA breast tumors to metastasize independent of the greater number of more aggressive tumors in this population?
Scientific Questions • Are there genetic susceptibility patterns that can be identified as being associated with the early onset of breast cancer independent of tumor type? • Is there a biological mechanism underlying the recent report suggesting that the incidence of advanced breast cancer in the AYA population has increased? [Johnson et al, 2013 JAMA 309 :800-805] • What mechanistic role does obestity play in early onset breast cancer? • Do AYA tumors show differences in tumor microenvironment that promote the development of more aggressive tumor types? • Are factors such as metabolism and micro-RNA different in AYA as compared to older patients, and can these factors be linked to tumor aggressiveness and poor therapeutic responses?
Next Steps for Adolescent and Young Adult OncologyBasic Biology-MelanomaSeptember 16-17, 2013
BBWG Members Magdalena Thurin Melinda Merchant Brandon Hayes-Lattin
AYA Melanoma • Melanoma is the 3d most common cancer diagnosed and the most lethal form of skin cancer among adolescents and young adults (aged 15-39 years) in the US. • The 5-year OS is 65% for regional and 15% distant metastatic site. • Melanoma incidence is higher among females compared with males. • Melanoma of the trunk are overrepresented in this age group. • Accuracy of melanoma cases reporting is limited because of incompleteness or nonspecific reporting including large proportion of unspecified histology. Known risk factors: • Adolescents and young adults appear to be at particular risk for developing melanoma because of UV exposure early in life. • Giant congenital nevi, neurocuataneous melanosis, xeroderma pigmentosum, Werner syndrome, retinoblastoma and immunosupression. • Transplant or chemotherapy for primary tumors. • Higher number of melanocytic nevi> 2mm in diameter. • Fair complexion, facial freckling, and family history of melanoma. • Understanding risk factors in AYA group is important to develop cancer control activities aimed at reducing melanoma incidence and death in this age group.
Biopathology of melanoma in the AYA population • The biopathology of melanoma have been the subject of controversy because of inability to distinguish conventional melanomas from a subgroup of melanocytic neoplasms with Spitz nevus-like morphology commonly seen in AYA patients. • Pathologically, these melanocytic lesions have spindle and epithelioid cell cytology, exhibit epithelial hyperplasia, giant melanocytes at the dermo-epithelial junction, various degree of pagetoid spread in the epidermis, Kamino bodies and others. • The outcome of melanoma in the younger, as compared to the older populations has been shown to differ substantially: • Metastases to sentinel nodes (SNL) are found more frequently in AYA groups with melanoma than would be expected in adults with the same stage of disease. • Melanoma in young patients is less likely to recur in distant organs. • Occurrence of more frequent LN metastases in young people suggests that melanoma cells in the young differ biologically and are more prone to progression and invasion.
Molecular studies • Comparative genomic hybridization (CGH) demonstrated multiple chromosomal aberrations in 95% of the melanomas with spitzoid morphology whereas typical Spitz nevi did not reveal more than an isolated gain in the region of chromosome 11 (11p). • The nevi that revealed an increase in 11p also showed frequent mutations in the gene encoding H-RAS(67%). • Spitz nevi lack the BRAFmutations that are common in melanocytic nevi and melanomas. • CGH may be used to distinguish spitzoid melanoma from Spitz nevus when pathological features are in question but the value of assessing mutations in the BRAF, N-RAS and H-RASgenes is not established for melanocytic lesions in AYA patients. • Spitz nevi as a group show high levels of p16expression. • A group of miRNA-regulators of cell growth, proliferation, invasion, and survival that is differentially upregulated in younger patients melanomas compared to adults has been recently characterized. miRNA-337-5p appear to be involved in cell growth and migration and targets Lyn TK. cyclin-D-1, D3, A and CDK4 are target genes of miRNA-let-7b that is overexpressed in AYA melanoma.
Challenges • AYA participation rates in clinical trials are drastically lower than for pediatric patients and also lower than for adults. • Few trials have enough AYA participation to have the statistical power to allow analysis stratified by age. • AYA continue to be treated under guidelines created for older adults. • Lower rates of medical comorbidities and polypharmacy may permit AYAs to tolerate higher doses of anticancer therapy. Therapy can be optimized at the highest-dose treatment level such as high dose IL-2 and high dose interferon IFNa-2b. • Chemotherapy is poorly studied in this group. • The genetic and progression markers of melanoma in the young are likely also to differ from those in melanoma of elderly populations, but this has yet to be studied. • The different biology of melanoma in AYA population suggests that the outcomes for younger patients may be improved over those of adults but the outcomes need to be studied in clinical trials of adequate size and maturity, with stratification for age.
Sarcoma • From the Greek sarx meaning "flesh“ • Cancer that arises from transformed cells of mesenchymal origin. • Bone, cartilage, fat, muscle, vascular, neural supportive tissues, soft tissue, etc. • Molecularly and clinically heterogeneous group: >50 types; rhabdomyosarcoma, Ewing’s sarcoma, osteosarcoma, chondrosarcoma, synovial, liposarcoma, desmoplastic small round-cell tumor, clear cell sarcoma, etc. • Incidence varies with age and diagnosis
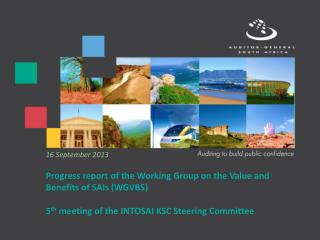
Survival rate is lower for AYA with Ewing’s sarcoma Modified from: Bleyer, A., Barr, R., Hayes-Lattin, B., Thomas, D., Ellis, C., and Anderson, B. 2008. The distinctive biology of cancer in adolescents and young adults. Nat Rev Cancer 8:288-298.
Sarcoma-BiologyMany driven by fusion oncogenesFunction of most unknown: Transcriptional/Epigenetic Action
Sarcoma-BiologyChallenges and Opportunities • Fusion genes are drivers for many sarcomas • Ideal targets because not expressed in normal tissues • Likely that fusion genes alter signal transduction, cell cycle progression, transcriptional regulation and epigenetic modification. Heterogeneous group and function of majority of largely unknown. • Difficult to target fusion genes if their primary role transcriptional regulation. Basic science research is needed. • The other genomic alterations aside from fusion genes, are largely unknown. >3000 tumor samples have been reported in sequencing studies 0 of them are AYA Sarcoma • Metastatic AYA sarcomas difficult to treat, largely chemo- insensitive. • Difference between AYA and childhood sarcomas unknown • Lack of animal models for AYA sarcoma
Current studies investigating the molecular characterization of this tumor type in the AYAO age group • Individual laboratories including the NCIs intramural program are performing next generation sequencing of Rhabdomyosarcoma, Osteosarcoma (largely pediatric) • NCI has completed a screen for a direct inhibitor of the EWS-FLI1 transcription factor • NCI is launching a screen for a direct inhibitor of the PAX3-FOXO1 transcription factor. • NCI trial NCT01109394 enrolls AYA patients for comprhensive “Omics” studies • NCI trial: Cediranib, in patients with ASPS demonstrated an overall response rate of 35% with a disease control rate of 84% at 24 weeks.
Are there specific molecular targets in this tumor type in AYAO patients that make it more vulnerable to specific therapeutic treatments. • PARP-1 inhibition trials in EWS underway. • Mithramycin was found to directly inhibit the EWS-FLI1 transcription factor scrreeing by high throughput; NCI trial open. • EWS-FLI1 fusion gene requires binding to RNA helicase A for oncogenic function. Strategies to inhibit interaction with RNA helicase A are underway. • Novel agents targeting the MET and VEGFR therapy pathway for tumors (ASPS) carrying the ASPL-TFE-3 fusion transcript ; e.g. a trial with caboxantinib, a dual inhibitor of VEGFR and MET, in these patients is underway [NCT01755195].
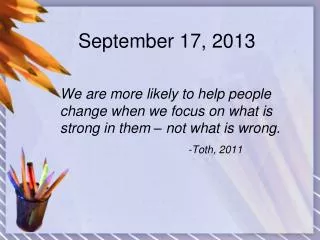
Massively Parallel Sequencing (Next-Generation Sequencing) Genomic DNA or RNA Fragmentation Fragment Size Selection DNA Fragments of Similar Sizes Adaptors Ligation Genomic DNA Library Amplification and Sequencing Align (Map) Reads to Ref. Genome Ref. Genome Genome Sequence AGCTGCTCGTCGCGAAACTCCGATCGACTGCTGATCGACTCGATCACTCGATCGTAGTCGAGAGTACTCGATGCT
Genomic Landscape of AYA Sarcomas:What is known? ? >3000 tumor samples have been reported in next generation sequencing studies 0 of them are for AYA Sarcoma
Genomic Approaches for the Comprehensive Analysis of the AYA Cancer Genome- Catalog “ALL” the Changes in the Genome DNA Whole Genome Genome Partition (e.g. Whole Exome) Epigenetic Landscape Messenger RNA Non coding RNA microRNA Other Gene Expression Fusion Genes Splice Variants Novel Transcript Expressed Mutations Copy Number Gene Rearrangement Epigenome Damaging Mutations Biomarkers: Diagnostic & Prognostic Biology: Drivers Therapeutic Targets: Mutations or Over Expressed Genes RNA Germ line Tumor Next Generation Sequencing
Next Generation Sequencing of Rhabdomyosarcoma (RMS): Fusion Positive RMS Have Lower Somatic Mutations Rate Implications Fusion Gene is the Driver Other Driver Mutations in fusion negative sarcoma
ARMS by histology, no PAX3/7-FOXO1 fusion detected, low mutation rate
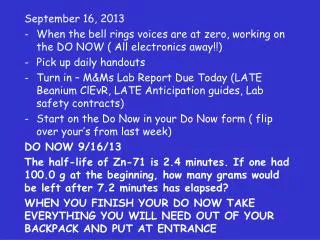
Fusion Negative ARMS Shows massive 2q Rearrangement with in-Frame PAX3-INO80D Purple:tail-to-head Green: head-to-tail junction (possibly tandem duplication) Orange: tail-to-tail junction or head-to-head junction (inversion)
RNAseq Confirms Expression of PAX3-INO80DNovel Fusion Transcript
SarcomaFuture Directions • Rare heterogeneous tumors, small numbers, requires a national/international strategy • Tumor bank that systematically collects blood, serum, plasma, fresh frozen tumor and FFPE tissues with clinical information database is required. • Next generation sequencing project and other “Omics” studies should be undertaken to catalog all genomic changes begin with exome and transcriptome • Biological function of fusion genes • Direct inhibitor of the fusion genes • Novel drugs/therapeutic strategies