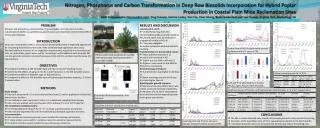
Addressing Barriers in CFS/ME Management: Recommendations for Canada
Explore the challenges faced in managing Chronic Fatigue Syndrome/Myalgic Encephalomyelitis (CFS/ME) in Canada and proposed solutions. Recommendations include training for healthcare practitioners, research funding, and establishing Centers of Excellence.

Addressing Barriers in CFS/ME Management: Recommendations for Canada
E N D
Presentation Transcript
Overcoming Systemic Barriersto Effective Management of Chronic Fatigue Syndrome/Myalgic Encephalomyelitis (CFS/ME) in Canada Marj van de Sande Grad Dip Ed Advisor & Webmaster, National ME/FM Action Network (Canada) mvandes@shaw.ca Clara Valverde BSc, RNFounder and Manager,Equipo Aquo (Spain) formacionsalud@hotmail.com Eleanor Stein MD FRCP(C) Calgary, Alberta espc@shaw.ca Alison Bested MD FRCP(C) Toronto, Ontario 416 283-0007 Patricia A. Fennell MSW LCSW-R Albany, NY www.albanyhealthmanagement.com Patients in Canada report long waiting times to get a diagnosis of CFS/ME. There is no effective treatment for CFS/ME. Why is this and how can it be rectified? Solution: Every physician and medical student in Canada should receive a copy of the Guidelines Health Canada should collaborate with provincial health departments, medical schools and medical and allied health organizations to ensure every health practitioner in Canada has adequate training forCFS/ME The Canadian Consensus Guidelines should be recognized as the standard of care in Canada. PROBLEM # 3 PROBLEM # 4 Why CFS/ME is Low on the Illness Prestige Hierarchy? Chronic conditions with less visible treatment procedures are at the bottom of the illness prestige hierarchy. (Album et al, 2007) CFS/ME is a newly recognized physical syndrome.However, some doctors don’t believe in CFS/ME. The seriousness of CFS/ME is underestimated. It is not viewed as serious or life threatening. CFS/ME patients’ quality of life is in fact seriously affected. (Hardt et al, 2001). CFS/ME the syndrome is often confused with Chronic Fatigue, the symptom. In fact CFS/ME can be distinguished from CF by using the international diagnostic criteria (Bombardier & Buchwald, 1995). CFS/ME is more common in women and women's complaints tend not to be taken as seriously as those of men (Richman et al, 2000). CFS/ME is viewed by some as an "illness" rather than a disease (Lloyd et al, 2000). In fact diagnostic tests are being developed (Kerr et al, 2007). Multisystem disorders cause physicians to experience disbelief and insecurity (Yunus, 2004). They are not supported by other medical doctors when they treat CFS/ME patients • Lack of Research Funding for CFS in • Canada • Research funding is urgently needed to identify: • better laboratory & diagnostic tests • measurement tools for the severity of the illness • & the degree of disability • better treatment options • genomic profiles • long term prognostic studies • long term sequelae • The CIHR web site shows three funded studies which include subjects with CFS/ME. From these there are two publications mentioning CFS/ME. • The AHFMR does not list any funded studies of CFS/ME. • Solution: • Develop a Centre of Excellence for CFS/ME to combine clinical care with research to advance our understanding and disseminate information to other providers. Make this a role model for centres across Canada. • CIHR should identify CFS/ME as a research priority and not an “orphaned illness”. • CIHR should, in collaboration with stakeholders, establish a Canadian research strategy for CFS/ME. METHOD Research has not been done in the Canadian health care system on the difficulties CFS/ME patients have accessing medical care. The conclusions in this poster were drawn from a survey of: recent medical literature, the experiences of patients of Dr. Stein and Dr. Bested, medical colleagues with expertise in CFS/ME (Canada and worldwide), the National ME-FM Action Network, and international consumer advocates. PROBLEM #2 • The Canadian Health Care System is • notdesigned to treat patients with • Complex Chronic Disorders. • Family Doctors and Specialists are not adequately compensated to work with patients who have chronic, multiple concurrent symptoms. • Specialists are expert in one body system. CFS/ME affects every body system. • CFS/ME has not been included in any Chronic Disease Management Program in Canada. It is an invisible illness. • Solution: • Develop publicly funded, multidisciplinary centres of excellence such as the model used in cancer and pain treatment in all cities across Canada. Programs should include: outreach programs with home visitations by doctors & health care workers plus phone consultations for bedridden patients too ill to visit the centre. • Add a billing fee code for CFS/ME. In Ontario a new time based billing code "K037" which specifically allows patients with CFS/ME and FM to be seen in ½ hour time increments. • Engage non physician professionals with training in CFS/ME to assist at medical practices i.e.. including CFS/ME in Primary Care Network plans and the CHR Chronic Disease Management System plus legal aid to help to assist with disability insurance & housing problems. PROBLEM #1 Physicians in Canada have not been taught how to diagnose CFS/ME using published guidelines. In Canada, in 2003, an international group of experts under the auspices of Health Canada established evidence-based guidelines for assessment, diagnosis and management of CFS/ME. This document is available at: http://www.mefmaction.net/Patients/ ConsensusDocuments In 2006 an overview of the guidelines was published & is available through the web site. Health Canada nor provincial health departments have not distributed these guidelines to physicans Solution: To change this demeaning bias, strong messages need to be given from those in authority - The Colleges, Medical School Deans and Health Canada, CIHR that: Patients with CFS/ME deserve respect & care comparable to that given to patients with any other medical condition. Physicians have a responsibility to patients to educate themselves and provide a standard of care compatible with the Canadian Consensus Guidelines for the Diagnosis and Management of CFS/ME. EFFECT ON PATIENTS In Other Countries: U.S. - the CDC has undertaken a widespread CFS/ME public awareness campaign, with advertising, a website (www.cdc.gov/cfs) and a toolkit for health care providers. Norway - the federal health minister stated in Parliament that CFS/ME was a serious health concern and the government pledged funds towards CFS/ME research. Spain - the patients of Catalonia gathered 140,000 signatures in support of a bill presented to the Catalan Parliament to improve access to care for patients with CFS/ME. See the quotes below for patient experiences CONCLUSIONS In Canada there needs to be: physician education, diagnosis of patients, establishment of centres of excellence, new billing fee codes and research on CFS/ME. Canadian patients deserve increased access to their own medical system and compassionate support from the health care system.