GI system
GI system. GI system consists of: >Gastrointestinal tract >Alimentary canal >Several accessory organs >Alimentary canal provides routes of intake

GI system
E N D
Presentation Transcript
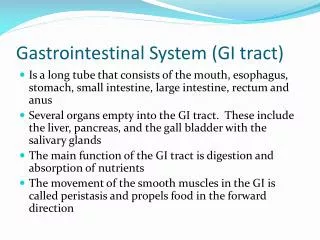
GI system • GI system consists of: >Gastrointestinal tract >Alimentary canal >Several accessory organs >Alimentary canal provides routes of intake for nourishment, digest, absorb nutrients, and eliminate waste. Consists of mouth, pharynx, esophagus, stomach, small intestine, and large intestine.
GI System • Accessory organs: >salivary glands, pancreas, liver and gallbladder . >Variety of radionuclides are available for evaluation of the GI tract, and specific organs.
Gi system • Salivary gland imaging is also known as nuclear sialography >salivary glands indiscriminately trap a number of ions and iodides >Tc99m pertechnetate is actively excreted by glands >production and excretion can be evaluated by using Tc99m
GI system • No patient prep needed • Patient seated facing camera • LEAP collimator • 1-5 mCi Tc99m injected. • Dynamic images acquired 1-2 sec per/fr. • Static images anterior, laterals • Lemon juice (diluted) is “swished” in mouth • Additional views are obtained to see washout of Tc99m from salivary glands
Gi system • Esophageal transit studies useful as non-invasive screening for esophageal motility disorders. • Good for esophageal motor disorder, not good for anatomic detail. • Barium swallow or endoscopy better for anatomical detail
Gi system • Imaging procedure: >2 hrs NPO >mix 300uCi Tc99m sulfur colloid in 15ml water >patient placed supine, anterior thorax placed under camera with stomach in FOV. >radiopharmaceutical administered through straw, entire volume held in mouth until instructed to swallow.
Gi system • Imaging procedure: >imaging begins, patient told to swallow >imaging is acquired at .25sec per/fr for 1min >15sec per/fr for remaining 9min >patient told to swallow continuously for entire test.
Gi system • Gastroesophageal reflux • Imaging procedure: >NPO for 8hrs prior to study >300uCi Tc99m sulfur colloid in 150ml orange juice and 150ml 0.1 hydrochloric acid >patient fitted with abdominal binder.
Gi system • Imaging procedure: >positioned supine under camera >binder cuff increased at different intervals >imaging begins no more than 10mins after drink is ingested >imaging occurs for 30sec at different inflation intervals 0, 20,40 etc.
Gi system • Gastric emptying studies are done to evaluate the function and motility of the stomach • When other radiographic or endoscopic exams cannot explain clinical signs • Mechanical and nonmechanical motility disorders can be summarized on Pg 457 table 16-1
Gi system • Imaging procedure: >patient must be NPO 8hrs prior >in-vivo and in-vitro labeling of chicken liver >500uCi Tc99m sulfur colloid injected into two raw eggs than cooked >patient eats cooked egg sandwich. >liquid portion is prepared with 125uCi of In111 in tap water.
Gi system • Patient eats and drinks both prepared substances • Imaging begins with camera peaked at two energy settings In111 and Tc99m • Images last for 60sec at both energies • Taken every 15mins for 2hours. • ROI drawn around stomach and counts are generated for each image.
Gi system • Gastric emptying using Tc99m sulfur colloid (solid phase) Tc99m-DTPA (liquid phase) • Same prep and imaging protocols different. • Gastric and Liquid phase done separately • Allergy to eggs can use oatmeal, baby food, sweet potatoes, beef or chicken liver.
Gi system • Dynamic or static imaging • Dynamic 60sec/fr for 60-90min • Static 60-120sec per/fr every 5mins for 30min. Every 15mins there after, for up to 3hrs. • Patient in supine position acquisition started as soon as patient is done eating. • Upon completion ROI drawn around stomach and counts are generated.
Gi system • Liver and Spleen imaging: >evaluation of functional liver disease such as, cirrhosis, hepatitis, and metabolic disease. >evaluation of hepatic lesion for biopsy, hepatomegaly, jaundice, ascities, and liver enzymes abnormalities.
Gi system • Liver and Spleen imaging: >Tc99m sulfur colloid and Tc99m albumin colloid most commonly used radiopharm. >large FOV used to image liver and spleen simultaneously. >Ga67 and Tc99m labeled RBC’s can also help for imaging certain lesions
Gi system • Liver and Spleen imaging: >good screening test with high sensitivity poor specificity. >no patient preparation. >should be done prior to iodinated or barium contrast. >barium can result in defects in the liver and spleen.
Gi system • Liver and Spleen imaging: • Adult dose= 5-10mCi sulfur colloid 1-8mCi albumin colloid • If flow study is needed: >position patient (xiphoid process at top of FOV) >inject and begin imaging immediately. blood pool image acquired after flow
Gi system • Liver and Spleen imaging: >15 min PI static imaging begins. >lead marker placed over last costal margin for liver >anterior, posterior, rt/lt laterals, anterior oblique (per protocol posterior oblique) >SPECT imaging acquired per protocol
Gi system • Liver hemangioma detection >Tc99m labeled RBC’s >most common benign tumor of the liver >discovered through CT or ultrasound >radionuclide technique generally 100% accurate >accurate diagnosis essential, inadvertent biopsy could lead hemorrhage
Gi system • Liver hemangioma imaging: >no patient prep, no radiographic contrast media in abdomen >post RBC’s labeling, bolus injection of 15-30mCi Tc99m tagged RBC’s is administered. >flow (dynamic) study is acquired 1/3 sec per/fr. Record blood flow >a blood pool image is acquired in anterior, posterior, RAO, RT lateral.
Gi system • Liver hemangioma imaging: >1-2 hrs PI SPECT imaging is acquired >planar (static) images may be acquired same projections as blood pool.
Gi system • Gallbladder (Hepatobiliary) imaging: >gallbladder concentrates and stores bile >located against the visceral wall of the gallbladder. >bile is received through common hepatic duct through the cystic duct >upon ingestion of a fatty meal, bile is discharged into duodenum to help break down food
Gi system • Gallbladder (hepatobiliary) imaging: >most common radiopharmaceutical agents: >Tc99m iminodiacetic(Tc99m-IDA) >Tc99m hepatoiminodiaetic (HIDA) >Tc99m DISIDA >Tc99m mebrofenin >I-131 rose bengal also used (no longer)
Gi system • Gallbladder (hepatobiliary) imaging: >investigating patients with upper abdominal pain >clinical indications: >acute or chronic cholecystitis >calculation of GBEF >evaluation of enterogastric reflux (bile) >evaluation of biliary surgery (bile leak) >jaundice >pediatrics: biliary atresia vs neonatal hepatitis >evaluation of “cold” defects on liver images.
Gi system • Imaging procedure: >patient NPO at least 2hrs prior >non-visualization of GB if not NPO >pain meds may interfere with transit of radionuclide. (morphine, opium ) >1-10mCi Tc99m-IDA agent given IV >imaging is began immediately >patient in supine position can be done sitting or erect
Gi system • Imaging procedure: >sequential images are obtained in the anterior projection for a minimum of 1hr. >gallbladder or biliary ducts fail to be visualized in 1hr imaging should be continued for up to 4hrs or longer. >CCK (cholecystokinin) or morphine may be needed in certain situations
Gi system • CCK is used to stimulate the gallbladder to contract when Biliary Dyskinesia is suspected • CCK aids in determining EF of gallbladder • Morphine is injected if cystic duct is patent and no visualization of gallbladder has happened.
Gi system • Gastrointestinal Bleeding: • Small intestine: >duodenum, jejunum, and ileum. >responsible for digestion, and absorption of all nutrients. >Large intestine: >cecum, ascending colon, transverse colon, descending colon, sigmoid colon, and rectum.
GI SYSTEM • Gastrointestinal bleeding indications: • Detect and localize bleeding sites >active or intermittent GI bleeds >caused by aspirin, ulcers, perforation, cancers, inflammation, diverticula, or angiodysplasia. > for detection patient must be actively bleeding.
Gi system • Gastrointestinal bleeding: • Radionuclide methods routine in most nuclear medicine departments. • In-vivo and in-vitro tagging. • Tc99m sulfur colloid • In-vivo PYP (pyrophosphate) tagged with 20-30 mCi Tc99m. • In-vitro labeled RBC’s (Ultratag) tagged with 20-30 mCi Tc99m
Gi system • Tc99m SC sulfur colloid 10-20 mCi administered • Most common in-vitro tagged RBC’s >1-3ml patient blood is tagged (ultratag) with 20-30mCi Tc99m >flow may be acquired if actively bleeding >static imaging 5,10,15,20, etc. to 60 mins >if no bleeding site located delay images may be needed
Gi system • Gastrointestinal bleeding: >dynamic imaging preferred >continuous images acquired at 60sec per/fr for 1hr. >delayed images needed if bleeding site not located after 1hr images >delayed images can be acquired up to 36hrs. >additional views laterals, oblique may also be needed to visualize bleed.
Please stop……. • ANY QUESTIONS?????? • LIGHTS !!!!!!!