Download
1 / 33
330 likes | 453 Vues

E N D
1. Introduction to Pandemic Influenza Vaccine and Antiviral Decision Issues
3. Key Vaccine and Antiviral Issues Approach to vaccine purchase and distribution (role of the public and private sectors)
Priority groups for receipt of pandemic vaccine
Priority groups for antiviral drugs and drug use strategy (chemoprophylaxis & therapy)
4. Pandemic Influenza Vaccine Production Timelines Development of reference strain
Use of reverse genetics allows HA and NA from pandemic strain to be combined with other genes from a strain well adapted to growth in eggs
Vaccine production (monovalent)
Master seed developed from reference strain
Growth in eggs and purification
Formulation and filling
Regulatory process
Optimal timing ~3 months (if reference strain and potency testing reagents already developed)
5. Pandemic Spread and Seasonality Spread of a pandemic
Months before U.S. community outbreaks for prior pandemic strains
1918 � 0; 1957 � 4-5; 1968 � 2-3; 1977 � 3-4
Spread of the next pandemic
More rapid because of increased international travel
More warning because of better surveillance
Seasonality
Fall � Spring seasonality generally preserved
Multiple pandemic waves occur � potentially in the same season
6. Asian Influenza in the U.S., July 1957
8. Influenza by Week of Onset in U.S. Counties, Fall 1957
9. Timeline of First and Second Pandemic Waves, 1957-58
10. Pandemic Vaccine Availability in Prior Pandemics
11. Vaccine Availability for the Swine Influenza Program
12. Pandemic Influenza Vaccine Supply Estimates: Current Status Pandemic vaccine supply assumptions
Only US produced vaccine will be available (1 mfr)
15 ug antigen/dose and 2 doses/person will be needed for protection
Monovalent vaccine production capacity will be 3-fold that of annual vaccine (e.g., similar Ag yield/egg)
Current Sanofi production is sufficient to deliver ~250 M monovalent doses/year (~5 million/week)
Implication � about 1% of the population can be protected per week
13. Pandemic Vaccine Purchase and Distribution Should vaccine purchase and distribution in the next pandemic be...
Similar to 1957 and annual influenza vaccination with most doses distributed in the private sector; or
Similar to 1976 Swine influenza program when vaccine was purchased and distributed by the public sector; or
Some other model?
14. Pandemic Vaccine Purchase & Distribution: Stakeholder Meetings, 2002 Series of individual discussions and meetings with stakeholders, coordinated by CDC
Objective to make recommendations on vaccine purchase and distribution to help state health departments in planning
Issues considered included ability to target supply, equity, cost, feasibility of implementation, and others
15. Pandemic Vaccine Purchase & Distribution: Stakeholder Meetings, 2002 Options considered
Primarily private sector program similar to inter-pandemic influenza seasons
Federal purchase for �traditional� public health care recipients (uninsured, military, children eligible for VFC) � est. 40-50 M
Federal purchase for above, HCWs, essential workers, and persons at high risk � est. 130-140 M
Federal purchase of all pandemic influenza vaccine
16. Pandemic Vaccine Purchase & Distribution: Stakeholder Meetings, 2002 Most stakeholders preferred the federal purchase option
Greatest equity; avoids price inflation; best targeting
This option was recommended for the first pandemic year only
Recommended negotiating a fair price and providing liability protection to manufacturers and those administering vaccine
17. Vaccine Purchase and Distribution: Potential for Changes Over Time
18. Reconsideration of Vaccine Purchase and Distribution Recommendations Experience since 2002
Release of draft HHS pandemic plan and progress in State pandemic planning
Experience with influenza and other vaccine shortages
Expansion of influenza vaccine recommendations for inter-pandemic seasons
Potential alternate approaches to consider
19. Inter-Pandemic and Pandemic Vaccine Target Groups Inter-pandemic vaccine recommendations
Persons at high risk of severe influenza & complications
Persons who can transmit disease to those at high risk (HCWs and family members of high risk)
Pandemic considerations
Pandemic impacts may extend beyond health of infected persons
Need to maintain quality health care system
Need to maintain essential community services
Vaccine supply will be more limited relative to need
20. Potential Vaccine Target Groups and Population
21. Questions in Defining Pandemic Vaccine Priority Groups How should response goals be balanced?
Can strata be identified within priority groups?
How does one define essential workers?
Should priority groups differ in more and less severe pandemics?
How should direct vs indirect vaccine effects be considered?
How should ethical issues and public preferences be considered?
22.
23. Goals and Principles of Influenza Antiviral Drug Use Goals of antiviral drug use
Decrease health, economic & social impacts
(Prevent a pandemic through intensive intervention in a cluster of a less efficiently transmitted strain)
(Slow disease spread early in a pandemic)
�Overarching principles�
Target drug to priority groups
Maintain flexibility and responsiveness to local needs
Consider efficiency in drug use strategies
Use drugs appropriately to limit wastage & resistance
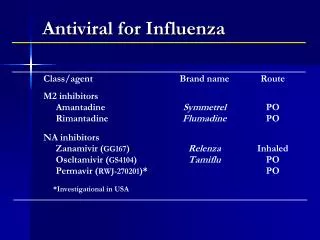
24. Influenza Antivirals Adamantanes � amantadine & rimantadine
Effective as prophylaxis; treatment shortens illness
H5N1 isolates from human cases in Asia resistant; resistance develops rapidly if used as therapy
Adverse events (neurological and GI) common
Produced by proprietary & generic manufacturers
Neuraminidase inhibitors � oseltamivir & zanamivir
Effective as prophylaxis; treatment shortens illness and reduces complications
Resistance uncommon
Few adverse events
Produced by proprietary manufacturers
25. Advantages of NIs for Antiviral Interventions in a Pandemic Documented effectiveness in decreasing influenza complications
Low rate of antiviral resistance and less risk of resistance spreading with widespread therapy
Low incidence of adverse events
Oseltamivir - orally administered, simple dosing, few contraindications (infants <1 year old)
26. Pandemic Antiviral Supply Global NI production capacity insufficient to meet pandemic needs � requirement for stockpiling
Antivirals in the Strategic National Stockpile
Oseltamivir (~2 million courses)
Rimantadine (~4 million courses)
Antivirals in the private sector
~1-1.5 million oseltamivir courses pre-influenza season
27. Critical Factors in Defining Drug Use Strategy: Prophylaxis vs Treatment Effectiveness � impact on health outcomes and social & economic function
Efficiency � optimal use of a limited antiviral supply
Feasibility � can the recommended approach be implemented?
Acceptability � is the approach ethical and acceptable to the public?
28. Number of Antiviral Drug Courses for Prophylaxis vs Treatment
29. Prophylaxis vs Therapy In Occupational Settings: Critical Unknowns Need for prevention (vs therapy) to avoid absenteeism
From illness
From fear of infection
Risk of transmission in occupational settings
E.g., from HCWs to co-workers and patients
Implementation factors
Ability to implement early therapy
Ability to assure availability of therapy
30. Target Groups for Antiviral Drug Interventions Priority groups are not defined in the draft pandemic plan
Establish priorities based on pandemic response goals
Draft report developed by an HHS/DoD/VA working group proposes priority groups for antiviral drugs
Represents conclusions from the working group and not HHS or its agencies
31. Cumulative Antiviral Courses for Proposed Groups by Pandemic Severity
32. Questions in Defining Pandemic Antiviral Priority Groups Similar questions as for vaccines (balancing goals; stratifying within groups; defining essential workers; ethical issues and public preferences; differences based on pandemic severity)
Will treatment be adequate to maintain health care and community services or will prophylaxis be needed?
How do implementation issues affect definition of target groups?
What drugs should be stockpiled and how does this affect definition of target groups?
33. Conclusions: Products of the Working Group & Subgroups Recommendations on approach to vaccine purchase and distribution, and on vaccine and antiviral strategies and priority groups are important for effective planning
Analysis of these issues by the PIWG and recommendations through NVAC and ACIP will facilitate decision-making and an effective pandemic response