Download
1 / 23
230 likes | 269 Vues
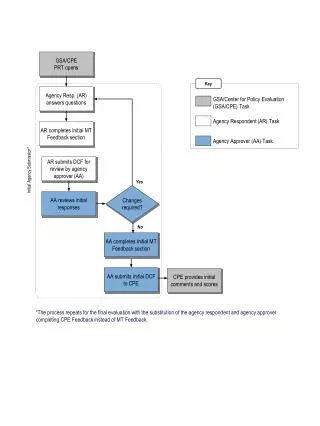
Therapeutic Strategies. PO 2 ???. Rebreathing Electrolytes/ECG monitoring. RESP ALKALOSIS. Sedation. Therapeutic Strategies. PO 2. PO 2. Rebreathing. PCO 2. RESP ALKALOSIS. RESP ACIDOSIS. permissive. Electrolytes. pH. Sedation. NIV/MV. ….Hypoxia kills…..Hypercarbia does not….

E N D
Therapeutic Strategies PO2 ??? Rebreathing Electrolytes/ECG monitoring RESP ALKALOSIS Sedation
Therapeutic Strategies PO2 PO2 Rebreathing PCO2 RESP ALKALOSIS RESP ACIDOSIS permissive Electrolytes pH Sedation NIV/MV
….Hypoxia kills…..Hypercarbia does not…. Hickling ICM 1989
Hypercapnia: clinical relevance and mechanisms of action …but consider pH….& Target Organs Curr Op Crit Care. 2015;21(1):7-12
Permissivity NOT allowed “mixed” pH 7.08 PCO2 70 HCO3 20
CPAP vs BIPAP vs MV ….There is always PEEP !!!!!!!!!!!!
THE BEST PEEP VD Alveolar recruitment and PaO2 DO2 low moderate high PEEP
H-L INTERACTIONS …….ifwhen the PEEP goes up, the BP goes down… The HEART ispreloaddependent…givefluids !!!!!!!!!!
NIV vs ETIin respiratoryacidosis TOO EARLY TOO LATE 2 hours Trial plus LACTATE CLEARANCE
Therapeutic Strategies PO2 PO2 PCO2 RESP ALKALOSIS RESP ACIDOSIS rebreathing permissive pH sedation NIV/MV fluids Electrolytes ( K, Mg, Ca) MET ALKALOSIS acetazolamide surgery
Total body water young b.w. 60% MEN elderly 50% WOMEN young 50% elderly 40%
70 Kg MAN ICF = 28 L ECF = 14 L 1/3 intravascular 2/3 interstitial 70% veins 18% arteries 3% arterioles
Persistance of fluids in blood after 60 minutes • 5% dextrose = 5% ? = • Cristalloids = 16% • Colloids = 30-50% Circulating volume • Albumin = 75-100% FIRST………….TEST !!!!
Therapeutic Strategies PO2 PO2 PCO2 RESP ALKALOSIS RESP ACIDOSIS rebreathing permissive pH sedation NIV/MV fluids electrolytes MET ALKALOSIS MET ACIDOSIS perfusion acetazolamide N surgery
IS A LOW pH BAD ? • CAN ALKALI RAISE pHi ? • IF (VENOUS) pH IS RAISED BY NaHCO3, IS THERE ANY SALUTARY EFFECT ? • DOES NaHCO3 HAVE NEGATIVE SIDE EFFECTS? CHEST (2000) 117: 260-67
PCO2 The CO2 lung presentation & low flow A V O2 demand DO2 VO2 ATP AMP + H+ Lact- + H+ H+ + HCO3-
BICARBONATE YESNO • HYPOPERFUSION • CARDIAC ARREST • HYPERCAPNIA • HYPOK, HYPOMg, HYPOCa • … • LOSSES • RENAL FAILURE • HYPERKALEMIA • INTOXICATIONS • RABDOMIOLYSIS • DKA ? • DYE ? • …………..
Four steps in hypoperfusion • best filling • best vasculartone • inotropes • ↓ VO2 + MV • Advanced options(ACP,VAD…)
Key points • In Respiratory disorders : first O2, then pH/PCO2, permissivity? • In Metabolic Alkalosis: (US-guided) filling & electrolytes • Colloids / Cristalloids / Both……?( think of deresuscitation) • In Metabolic Acidosis …look at perfusion