HIV in Pregnancy and Its Management
280 likes | 324 Vues
Learn about the impact of HIV on pregnancy, transmission rates, diagnosis methods, and comprehensive antepartum care strategies to reduce vertical transmission risks. Discover the latest NACO guidelines for managing HIV-infected pregnant women.

HIV in Pregnancy and Its Management
E N D
Presentation Transcript
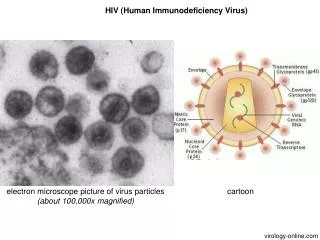
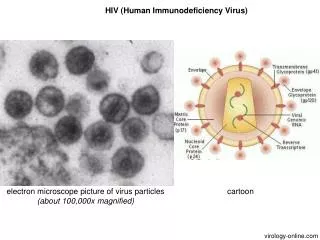
HUMAN IMMUNODEFICIENCY VIRUS In pregnancy
Introduction • Global epidemic • UNAIDS 2010 – there is 19% reduction in HIV infected people. • 20% reduction in AIDS related death • Number of women affected has risen to 50%
Millennium development goal 6 aims to decrease new pediatric HIV infection and improve HIV-free child survival • India has the second highest population of HIV infected people • HIV is a retrovirus containing reverse transcriptase enzyme, which allows the virus to transcribe its RNA genome into DNA, then integrates into host cell DNA
RNA virus – sub gp of lentivirus • exists in two forms HIV-1 Common HIV-2 • HIV preferentially targets lymphocytes expressing CD4 molecule, causing progressive immunosuppression • Main problem in clinical illness with AIDs is profound immunosuppression rendering patient susceptible to opportunistic infections and neoplasia.
Modes of HIV transmission • Sexual route 8.6% • Mother to child 3.6% • Injection drugs 2.4% • Transfusion of blood 2% • Others 6%
DIAGNOSIS : • Elisa test is used for screening test – becomes +ve within 3 weeks to 3 months after exposure. • Previously a +ve test needed confirmation with either western blot / immuno fluorescence • PCR detects viral DNA / RNA • CD4 counts decline indicates degree of Immuno suppression • Viral load (HIV – RNA) predicts disease progression
Effect of pregnancy on HIV • Does not increase the risk of progression of HIV. • Women with advanced disease may deteriorate • Opportunistic infections may be less aggressively investigated
Effect of HIV on pregnancy : • In advanced disease, increased risk of miscarriage, PTL, IUGR • Main concern is vertical transmission
Vertical transmission Varies between 15-20% in non BF women Europe 25-40% in African population India 30% Antepartum 0-14wk 1% 14-36wk 4% >36wk 12% Intrapartum 8% Postpartum established 14% priinf 29%
Factors increasing vertical transmission • H/O previus child with HIV • Maternal viral load • Seroconversion in pregnancy • Advanced maternal disease • Low CD4 count • Prolonged ROM • First born twin
Factors increasing vertical transmission • PTL • Chorioamnionitis • Coexistent STD • Antepartum invasive procedures • Intrapartum invasive produces • Episiotomy,lacertions, • Forceps delivery • Breast feeding
Preconceptional management • Couples who are serodiscordant – use condom • Female partner (HIV –ve) should be advised that assisted conception with either donor inseminate or sperm washing • Couples should be advised to delay conception until viraemia is suppressed • All women who are HIV +ve are recommended to have annual cervical cytology cytology
ANTEPARTUM MANAGEMENT • Multidisciplinary team management • PPTCT was commenced in 2002 • Screening offered to all pregnant mothers. • Pretest and post test counselling are mandatory • Women who decline HIV test – are eligible to receive all ANC benefits are known as ‘opt out’.
Screening all pregnant mother in early pregnancy • Screening offered again at round 28 weeks • ART should be offered to all pregnant women who test +ve for HIV infection (maternal health/vertical transmission
ANC : Termination should be discussed at the earliest • counselled regarding nutrition, hygiene, safe sex, avoid substance abuse. RFT, LFT, viral load. CD4 count – Rpt 3mnths • Screening for genital infection done early Rpt at 28 wks. . Hepatitis and pneunococcal vaccines is recommended
NACO revised guidelines • All HIV infected pregnant women should be initiated on life long ART regardless of WHO clinical stage or CD4 count/ gestational age. • HIV infected pregnant mothers should preferably be initiated on ART at ART centres and should not be delayed for want of CD4 cell count report.
NACO revised guidelines • The three drug option recommended are tenofovir(TDF)+ lamivudine(3TC) + efavirenz (EFV) Zidovidine(AZT) +3TC +nevirapine(NVP) AZT +3TC +EFV TDF +3TC +NVP • Mode of delivery should be vaginal, cs are done for obstetric reasons • Avoid ROM, Ergometrine , early cord clamping
NACO revised guidelines • Breast feeding – is discouraged • Bottle feeding may be more harmful in certain SE condition • Risk of neonate dying of diarrhoea has to be weighed against transmission of infection.
ARV • HAART : Benefits outweigh the risks • Deferred until 1st trimester • Include 2 nucleoside RTI with either one/non PI or non NRTI • Efavirenz is C/I as it can cause cong. Abnormalities
Regimen to continue after delivery • Women who conceive while on HAART should continue the same.
Neonatal care • All babies are Rx with ARV from birth (Zidovdine10 mg in 1ml suspension) is give for 6 weeks in non Breast fed babies. • In B Feed neonates – continues until one week after stopping B feeding. • Diagnose of infant HIV at birth can thro’ PCR/DNA analysis dried blood spot / blood in EDTA are specimens used to perform PCR
Care of HIV exposed infant • Exclusive breast feeding for six months • NVP prophylaxis from birth till 6 weeks • Cotrimoxazole prophylaxis from 6 weeks till 18 months • Early infant diagnosis (EID) of HIV – DNA – PCR testing (6 weeks, 6 months, 12 months or 5 weeks after stopping breast feeding and confirmation with antibody test at 18 months ) • Level of maternal antibody falls below the limit of detection by 18 months.
Regular immunization as per national schedule • Continued breast feeding and growth monitoring • Follow-up of child till 18 months for confirmation of HIV status
Antibody test can identify potentially uninfected infants 6-18 months of age if they are not breast fed. • A negative HIV antibody test at 18 months confirms that the child is not infected. • Children with known/suspected asymptomatic HIV infection should receive vaccines according to national immunization schedule.
Contraception • Barrier method
Universal precaution • Staff should adhere to universal precaution during delivery • Wear protective eye wear, mask, wear double gloves • Wear gown and protective leg wear
Universal precaution • Handle all linen soiled with blood fluid as potentially infections. • Process all lab specimen as PI • Wash hands before and after all patient or specimen contact • Place all used syringes immediate in nearby impermeable contained don’t recap or manipulate.
Measures to reduce vertical transmission • Universal screening • ARV in pregnancy • Exclusive formula feeding