Patient Individual Multiscale Geometric Modeling of the Tracheobronchial Tree
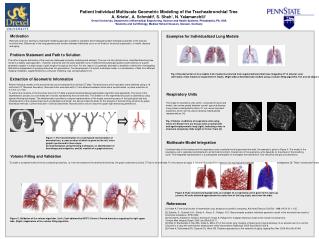
Develop a multiscale geometric model to represent individual properties of the lung's trachea-bronchial tree, extracted from clinical CT data with volume filling and graph integration techniques for personalized research.

Patient Individual Multiscale Geometric Modeling of the Tracheobronchial Tree
E N D
Presentation Transcript
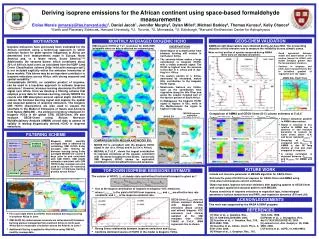
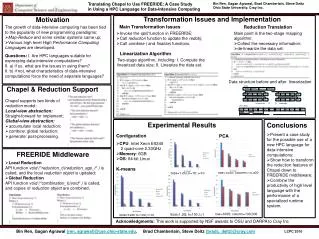
Examples for Individualized Lung Models Research goal is to develop a multiscale modeling approach suitable to represent and investigate patient individual properties of the trachea- bronchial tree. Differences in the lung geometry and function between individuals occur on all levels of structural organization, in health, disease and aging. Patient Individual Multiscale Geometric Modeling of the Tracheabronchial TreeA. Kriete†, A. Schmidt‡, S. Shah†, N. Yalamanchili††Drexel University, Department of Biomedical Engineering, Science and Health Systems, Philadelphia, PA, USA‡Anatomy and Cell Biology, Medical School Giessen, Giessen, Germany Problem Statement and Path to Solution The rather irregular dichotomy of the lung has challenged computer modeling and analysis. The use of a fully dichotomous, simplified branching tree model is a widely used approach. However, branches with the same diameter occur in different bifurcating generations and branches of a given generation appear in a wide range of path lengths throughout the hilum. For this reason it is generally desirable to establish a method for investigating distribution independent of grouping branches into generations. The development of a hybrid, multiscale model, in a combination of data from different imaging modalities, supplemented by a computer modeling, was conceptualized in [1]. Fig. 3 Reconstruction of tree models from 2 patients extracted from segmented bronchial trees imaged by CT in anterior view: (Left sides:) Tube models of segmented CT stacks. (Right sides:) Extended tube models using a volume filling algorithm. The overall shape of lung differs between individuals. Extraction of Geometric Information Patient individual models of the bronchial tree can be extracted from clinical CT-data. Thoracial scans at full inspiration were obtained using a 16 multi-slice CT (Siemens Sensation). Reconstruction was done with 0.7 mm distance between slices and a reconstructed in plane resolution of 0.7 mm x 0.7 mm. To extract the structure of the bronchial-tree from CT-data a special threshold based segmentation algorithm was applied [2]. The result of the segmentation process is a connected set of voxels representing the bronchial tree. The skeleton of the segmented structure is obtained by using special thinning techniques. The skeletonization provides a compact representation of the shape, preserving many of the topological and size characteristics of the original object such as diameter and length, but also provides the basis for the analysis of the branching structure by graph theoretical methods. Current resolution of clinical data allows reconstructions only for about the upper eight branching generations. Respiratory Units The shape of respiratory units (acini), composed of ducts and alveoli, also varies greatly between normal, age and disease. Lung tissues investigated by Micro-CT can reveal important properties, which can be used to develop individualized representations [4]. Fig. 4 Volume renditions of respiratory units using micro-CT. Shown here are tissues from a normal (left) and aged emphysematic lung (right), indicating a loss in structural complexity. Side length is 10 mm. From [5]. Motivation Figure 1: The transformation of a voxel-based representation of bronchial tree, a cross-section of which is given on the left, into a graph is performed in three steps: (b) skeletonization using thinning techniques, (c) identification of branchings and endpoints, and (d) creation of a graph structure. Multiscale Model Integration Combined data of the trachea and the respiratory units constitute the final geometrical model. An example is given in Figure 5. The model of the respiratory unit is replicated and attached to all terminal bronchioli. Overall size of the respiratory units depends on the phase of the breathing cycle. This integrated representation is a prerequisite prerequisite to investigate flow distribution, flow velocities and gas concentrations. Volume Filling and Validation To obtain a complete model of the air conducting branches, i.e. from the trachea to the terminal bronchioles, the graph obtained by clinical CT has to be extended. For this reason we apply a volume filling algorithm, based on the topological knowledge gained from previous investigations [3]. These “constructed” branches are generated into the individual lobar volumes, provided on the original clinical data. The algorithm fills lobular volumes by successive dichotomic branching until a volume of the size of a respiratory unit is reached. We have validated this method by using a cast model imaged with HRCT, as described in [3]. Figure 5: Fully reconstructed graph (left), an example of a respiratory unit is given in the zoom-up (center). All units attached approximate the outer form of the lung (right, seen from the side). References [1] Kriete A. Form and function of mammalian lung: analysis by scientific computing. Adv Anat Embryol Cell Biol. 1998;145:III-IX, 1-105. [2] Zidowitz, S., Schmidt, A.H., Kriete, A., Krass, S., Peitgen, H-O: Steps towards a patient individual geometric model of the bronchial-tree used for functional simulations. SPIE 2004 [3] Schmidt A, Zidowitz S, Kriete A, Denhard T, Krass S, Peitgen HO. A digital reference model of the human bronchial tree. Comput Med Imaging Graph. 2004 Jun;28(4):203-11. [4] Watz H, Breithecker A, Rau WS, Kriete A. Micro-CT of the human lung: imaging of alveoli and virtual endoscopy of an alveolar duct in a normal lung and in a lung with centrilobular emphysema--initial observations.Radiology. 2005 Sep;236(3):1053-8. [5] Kriete A, Sokhansanj BA, Coppock DL, West GB. Systems approaches to the networks of aging. Ageing Res Rev. 2006 Nov;5(4):43-48. Figure 2: Validation of the volume algorithm. (Left:) Cast obtained by HRCT. (Center:) Pruned bronchus supplying the right upper lobe. (Right:) Application of the volume filling algorithm.