Download
1 / 11
110 likes | 238 Vues
Presenter Mihail.Samnaliev@umassmed.edu, PhD Funded by: RWJ Foundation Substance Abuse Policy Research Program Grant: “Medicaid Beneficiaries with Co- occurring Disorders”, PI: Robin Clark, PhD Center for Health Policy & Research (chpr)

E N D
Presenter Mihail.Samnaliev@umassmed.edu, PhD Funded by: RWJ Foundation Substance Abuse Policy Research Program Grant: “Medicaid Beneficiaries with Co- occurring Disorders”, PI: Robin Clark, PhD Center for Health Policy & Research (chpr) University of Massachusetts Medical School Ethnic Disparities in Place of Service Among Medicaid Beneficiaries with Mental Illnesses
Rationale Accumulating evidence indicates that ambulatory care received by Afrc Amer and Hispanics with mental illness (MI) lags behind that received by White Americans with MI African American and Hispanics receive poorer access and quality of care (Miranda et al 2002); poorer preventive care and rely on hospitals more heavily than White Americans (MEPS, AHRQ) People with mental illness (MI) face barriers to receipt of care (Druss & Rosenheck 1998), are underdiagnosed (Kessler et al 2005), have greater rates of chronic co-morbidities (Felkeret al 1996); higher cost (Wolf et al 2002) Why Medicaid: - Very few national studies of Medicaid beneficiaries with MI - Medicaid MH expenditures = $24 billion in 2001 (DHHS 2005)
Study objectives Compare frequency of ambulatory care visits, for mental or co-morbid disorders, received by African, Hispanic and White Medicaid beneficiaries with MI, and if it affects health outcomes 1. Identify 12-month diagnosed prevalence of MI and ambulatory care sensitive (ACS) comorbidities among those with MI - Any MI; focus on 16 ACS conditions (e.g., asthma) 2. For each ethnic group, explore rates of physician office visits with a primary diagnosis of MI or ACS condition (e.g., a primary Dx of asthma means an office visit to seek care for asthma) 3. How does 2 relate to ACS (preventable) hospitalizations across States (Effects of state Medicaid Programs) ______ Ethnic/racial categories as defined in the Medicaid claims datasets for 1999
Methods and data • Quasi-experimental design: 6 states were selected from different regions of the U.S. • Logit models -> probability of office visits and hospitalization with • (i) MI (among beneficiaries diagnosed with MI), or • (ii) ACSC (among those diagnosed with MI + ACSC), or • (iii) any diagnosis (among beneficiaries diagnosed with MI) • Example: • How often did a Hispanic beneficiary, diagnosed with depression and asthma in 1999, receive care for asthma in (a) physician’s office vs. (b) hospital? Are (a) and (b) correlated ;does it vary by State? Why?
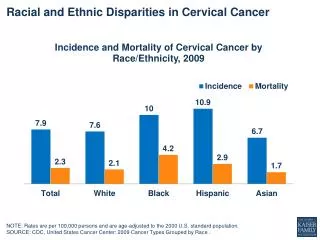
RESULTS A total of 4 million beneficiaries, including: 55% White, 30% African American, 6% Hispanic Of which 350,000 (9%) diagnosed with MI (12-month prevalence) Of which 176,000 (47%) diagnosed with one or more ACSC For example: 5% had MI and asthma 12% had MI and COPD 14% had MI and diabetes 23% had MI and hypertension
RESULTS (cont) • African Americans and Hispanics diagnosed with MI received care in office 2 times less often than White beneficiaries - including office visits with a diagnosis of MI, ACS or any Dx - suggests poorer preventive care for mental and co-morbid illness • Higher rates of hosp. for ACS or any diagnosis, but not for MI. - especially Afrc Amer with MI and ACSC - suggests worse health outcomes which may be caused by a lack of ambulatory preventive care _________ Aside: All results above apply to people diagnosed with MI, but it seems that rates of diagnosis are themselves affected by the lower rates of outpatient visits: African and Hispanic beneficiaries had up to 3 times lower diagnosed MI prevalence, quite different from the NCS, and the ECA which report similar rates across ethnic/racial groups
RESULTS (cont) There was significant interstate variations in rates of office visits and hospitalizations: - Pr(office visits) 0.4 to 0.9 - Pr(hospitalization) as much as 1.8 - In 5 states, Hispanic and African American had lower rates of office visits and non-significant or higher ACS hospitalization rates, particularly among Afrc Amer with MI & ACS - One state: equal ACSC office, and hospitalization were found between African and White Americans.
Summary Rates of ACS comorbidities ~ 50% for all ethnic groups Afrc Amer and Hispanics with MI were less likely to receive care in office-based settings, and more likely to be hospitalized In one state: equal rates of office-based care among the 3 ethnic groups and nonsignificant differences in rates of hospitalizations among the 3 ethnic groups Conclusion and Implications State Medicaid programs may be able to improve primary care and health outcomes for Afr Amer and Hispanics with MI by enhancing accessibility/use of care in office-based settings.
Appendix I: Odds Ratios1: office visits and hospitalization African American vs. White